ISSN : 1598-2939
ISSN : 1598-2939

© Korea Institute of Sport Science
This study examined the accuracy and consistency of hand-held dynamometer (HHD) in assessing leg muscle strength in older adults.
Forty-eight elderly men and women (12 males and 36 females), aged 60-85 years, were recruited for this study. All study participants had anthropometric measurements, handgrip, the HHD, and isokinetic dynamometer tests. Pearson partial correlations were used to examine the validity of HHD compared with an isokinetic dynamometer after adjustment for age, sex, and race. Cronbach α coefficients were used to estimate the test-retest reliability of the HHD measurement.
Age-, sex-, and race-adjusted partial Pearson correlation coefficients were 0.90 for isometric leg strength (p < 0.001), 0.62 for isokinetic leg strength (p < 0.001), and 0.63 for handgrip strength (p < 0.001) with the HHD. Cronbach α coefficients showed high interclass reliabilities in measuring leg muscle strength using the HHD in men (α=0.99) and women (α=0.96).
The HHD had good concurrent validity with high interclass reliability in assessing leg muscle strength in older adults.
This study examined the accuracy and consistency of hand-held dynamometer (HHD) in assessing leg muscle strength in older adults.
Forty-eight elderly men and women (12 males and 36 females), aged 60-85 years, were recruited for this study. All study participants had anthropometric measurements, handgrip, the HHD, and isokinetic dynamometer tests. Pearson partial correlations were used to examine the validity of HHD compared with an isokinetic dynamometer after adjustment for age, sex, and race. Cronbach α coefficients were used to estimate the test-retest reliability of the HHD measurement.
Age-, sex-, and race-adjusted partial Pearson correlation coefficients were 0.90 for isometric leg strength (p < 0.001), 0.62 for isokinetic leg strength (p < 0.001), and 0.63 for handgrip strength (p < 0.001) with the HHD. Cronbach α coefficients showed high interclass reliabilities in measuring leg muscle strength using the HHD in men (α=0.99) and women (α=0.96).
Age-related loss of skeletal muscle mass, muscle strength, and muscle quality is a major public health concern in the geriatric populations (Janssen, Heymsfield, & Ross, 2002; Yu et al., 2016). Approximately 30% of adults over the age of 60 suffer from sarcopenia (Baumgartner et al., 1998; Haehling, Morley, Anker, 2010; Janssen et al., 2002). Importantly, sarcopenia is primarily associated with physical disability and cardiovascular disease (Janssen et al., 2002; Ko et al., 2016; Seene & Kaasik, 2012). Thus, detecting muscle weakness and improving muscle strength in elderly populations is important to prevent falls, disability, and mortality.
The isokinetic dynamometer is a gold standard for measuring leg muscle strength although it is impractical in the field testing with high costs (Cooper et al., 2013). Alternatively, hand-held dynamometers (HHD) have been widely used to measure muscle strength across various populations with different health conditions (Deones, Wiley, Worrell, 1994; Kim et al., 2014; Lu et al., 2012; Reinking et al., 1996). The HHD is portable in measuring an isometric muscle strength at multiple angles and limbs. Nonetheless, the accuracy and consistency of the HHD in measuring muscle strength remains controversial. Several investigators have shown high validity of the HHD (r=0.91) in assessing leg muscle strength compared with isokinetic dynamometer (Martin et al., 2006), while other studies have also shown low validity of the HHD (r=0.34 – 0.57) (Deones et al., 1994; Kim et al., 2014; Lu et al., 2012; Reinking et al., 1996). These inconsistent findings may lead to confusion to the public and clinical settings as a screening to access muscle strength using the HHD. Importantly, there has been limited research on the validity of the HHD in older adults compared with an isokinetic dynamometer. We, therefore, examined the concurrent validity of HHD in assessing leg muscle strength against isokinetic dynamometer in older adults. We also assessed the interclass reliability of the HHD in older adults.
This study is a cross-sectional study with a repeated measurement design. Forty-eight elderly men and women (12 males and 36 females), aged 60-85 years, were recruited for this study using emails, phone calls, and fliers. Eligibility for study participation was determined through an online questionnaire, including PAR-Q+. All study participants had no personal history of heart disease, stroke, or cancer at baseline. All procedures were approved by the Arizona State University Institutional Review Board (IRB) and written informed consent was obtained from all study participants before study participation. All subjects were given a detailed description of the protocol prior to study participation.
Body height and weight were measured using a standard physician’s scale. Waist girth was measured at the midpoint between the anterior superior iliac crest and a lowest lateral portion of the ribs. Seated blood pressure was measured after 5 minutes of rest using a random-zero sphygmomanometer. Dual-energy X-ray absorptiometry (DEXA) was used to obtain body composition and arm and leg muscle mass by a licensed lab technician. The HHD (microFET2, portable digital HHD, Hoggan SCI, LLC, Salt Lake City, UT) was used to measure isometric knee extension strength (1 set of 3 repetitions) at an angle of 60 degrees. The distance from the ankle to the middle of the patella was measured to compute newton meter (Nm). The Biodex isokinetic dynamometer (System 4 ProTM) was used to measure isometric leg strength (Nm) (1 set of 3 repetitions) at an angle of 60 degrees and isokinetic leg strength (Nm) (1 set of 3 repetitions) at 180 degrees per second. The dominant leg was used for measurement. An average of the highest two performance scores was used for analysis. The grip strength was measured using the Takei Physical Fitness Test dynamometer. The dominant hand was used for measurement. Grip strength was measured twice, and the average of two test scores was used for analysis. All measurements, except for DEXA, were collected by one investigator to minimize measurement errors associated with instrument and rater.
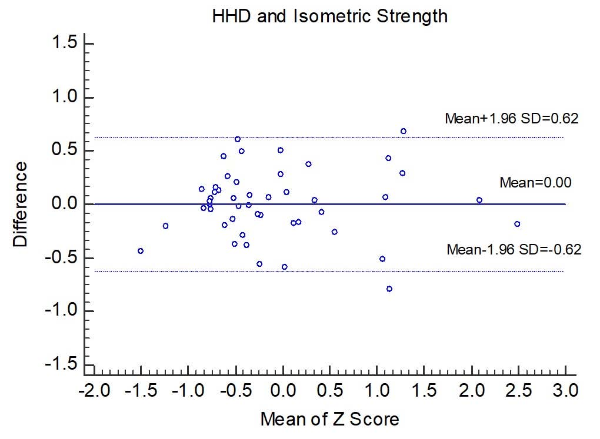
General linear models (GLM) were used to test mean differences for anthropometric, and systolic and diastolic blood pressure measurements between men and women. A χ2 test was used to test frequency difference by race. General linear models were also used to test statistical differences for the HHD and isokinetic dynamometer values between men and women after adjustment for age and race. Age-, sex-, and race-adjusted partial Pearson correlations were used to investigate the associations of HHD with an isokinetic dynamometer and handgrip strength. Cronbach α coefficients (Cronbach, 1951) were used to examine the interclass reliabilities of the HHD in assessing leg muscle strength. The standard error of measurement (SEM) was calculated as SD . We standardized all variables to z-scores and performed Bland-Altman plots, testing mean difference between the HHD and isokinetic dynamometer using one-sample a t-test. The proportinoal bias was tested using a simple regression analysis by comparing the difference and average scores between the HHD and isokinetic dynamometer. All statistical procedures will be performed by the Statistical Analysis Systems (SAS Institute).
Descriptive statistics are expressed as means and standard deviations (SD) in Table 1. Forty-eight participants responded to the online survey were eligible for the study. The study participants consisted of 12 males and 36 females, aged 60-85 years. Approximately 72 to 75% of study participants were whites in men and women, respectively.
| Men | Women | p value | |
|---|---|---|---|
| Age (years) | 69.8±7.0 | 68.6±5.9 | 0.55 |
| Height (cm) | 176.6±5.9 | 158.2±7.1 | <0.001 |
| Weight (kg) | 84.3±10.9 | 69.9±69.9 | 0.002 |
| BMI (kg/m2) | 27.1±3.5 | 27.4±6.3 | 0.88 |
| Body Fat (%) | 31.8±3.4 | 40.8±6.9 | <0.001 |
| Waist Girth (cm) | 101.8±4.9 | 89.3±12.4 | 0.002 |
| SBP (mmHg) | 138.3±15.3 | 133.7±15.5 | 0.37 |
| DBP (mmHg) | 77.5±9.7 | 81.7±7.7 | 0.13 |
| Race (whites, %) | 75 | 72.2 | 0.85 |
As shown in Table 1, males had greater mean scores for height, weight, and waist girth when compared to women (all p < 0.005), while females had greater body fatness than did males (p < 0.001).
Table 2 indicates age- and race-adjusted mean scores for handgrip, the HHD, and isokinetic and isometric leg strengths in men and women. Males had a greater age- and race-adjusted mean values for the handgrip strength (p < 0.001), the HHD (males, 146.7 Nm vs. females, 82.4 Nm, p < 0.001) and isokinetic (81.6 Nm vs. 41.5 Nm, p < 0.001) and isometric leg strengths (137.3 Nm vs. 76.8 Nm, p < 0.001) than did female counterparts.
| Men | Women | p value | |
|---|---|---|---|
| HHD (Nm) | 146.7 | 82.4 | <0.001 |
| Isometric (Nm) | 137.3 | 76.8 | <0.001 |
| Isokinetic (Nm) | 81.6 | 41.5 | <0.001 |
| Handgrip (kg) | 37.6 | 21.5 | <0.001 |
Age-, sex-, and race-adjusted partial Pearson correlation coefficients were 0.90 for isometric leg strength (p < 0.001), 0.62 for isokinetic leg strength (p < 0.001), and 0.63 for handgrip strength (p < 0.001) with the HHD as shown in Table 3. The HHD is highly associated with isometric leg strength, followed by isokinetic and handgrip strengths.
| HHD | Isometric | Isokinetic | Handgrip | |
|---|---|---|---|---|
| HHD (Nm) | 1.00 | |||
| Isometric (Nm) | 0.90* | 1.00 | ||
| Isokinetic (Nm) | 0.62* | 0.69* | 1.00 | |
| Handgrip (kg) | 0.63* | 0.73* | 0.60* | 1.00 |
Table 4 represents the interclass reliability with SEM for handgrip and HHD strength test scores in men and women. Cronbach α coefficients showed high interclass reliabilities in measuring the HHD in men (0.99) and women (0.96). There was also high interclass reliabilities for handgrip strength measurements in men (0.99) and in women (0.94).
| Men | Women | All | |
|---|---|---|---|
| HHD (Nm) | 0.99(6.13) | 0.96(4.48) | 0.99(4.40) |
| Handgrip (kg) | 0.99(0.90) | 0.94(0.41) | 0.99(0.88) |
As shown in Figure 1, Bland-Altman plots showed high agreement between the HHD and isokinetic dynamometer. There was no significant mean difference between the HHD and isokinetic dynamometer (p > 0.05). There was also no proportional bias for the difference scores across average scores between the HHD and isokinetic dynamometer (β = 0.057, p = 0.23).
Our major finding was that leg muscle strength estimated by the HHD had a high correlation with isometric leg strength estimated by isokinetic dynamometer in older adults. Our findings are consistent with UK elderly men and women study (aged 61 to 81 years), which showed good concurrent validity of the HHD (r=0.91) compared with isometric leg strength estimated by the Biodex (Martin et al., 2006). Other investigators have shown a moderate to high correlation coefficients between leg strength estimated by the HHD and isometric dynamometer (r=0.79 to 0.83) (Andrews, Thomas, & Bohannon, 1996; Bohannon, 1997). However, our findings are inconsistent with findings from other studies, which showed a weak association between leg strength estimated by the HHD and isokinetic dynamometer in healthy young adults (Kim et al., 2014; Lu et al., 2012) (r=0.41 to 0.47) or patients with knee dysfunction (Deones et al., 1994; Reinking et al., 1996) (r=0.34 to 0.57).
Our findings also indicate high interclass reliability in measuring the HHD in both men and women (reliability>0.96). Other studies have shown a moderate to high interclass reliabilities in measuring the HHD (reliabilities, 0.76 to 0.99) (Toonstra & Mattacola, 2013; Surburg, Suomi, & Poppy, 1992; Arnold et al., 2010). Some investigators have also shown poor instrument reliability using the HHD. According to Truesdale-Jackson and her associates (1994), the interclass reliability for two Nicholas HHD was 0.58 in healthy females, aged 20-56 years. Further studies need to examine the instrument reliability using the microFET2 HHD.
Our findings also documented that the HHD tends to slightly overestimate leg muscle strength when compared with leg muscle strength estimated by an isokinetic dynamometer. Our results are inconsistent direction with other studies, which showed that the HHD tends to underestimate muscle strength as compared with isometric leg strength (Toonstra & Mattacola, 2013; Arnold et al., 2010; Kim et al., 2014; Martin et al., 2006). Other studies have also shown that HHD tends to overestimate in patients with intellectual disabilities or patients with amputations (Surburg et al., 1992; Leijendekkers et al., 2017). Martins et al. (2017) pointed out that there are some possible errors in measuring the HHD when compared to an isokinetic dynamometer.
A strength of this study is that we used gold standard equipment for measuring quadriceps strength using the Biodex, which produces accurate and reliable measures for muscle torque (Feiring et al., 1990). Another strength is that we estimated the HHD leg muscle strength by attaching the HHD to the isokinetic dynamometer. Several studies have reported that there are some errors in measuring leg muscle strength without attaching the HHD to the isokinetic dynamometer causing instability of the tester (Hayes et al., 1992; Martin et al., 2006; Reed et al., 1993). Our study minimized this error by physically attaching the HHD to the isokinetic dynamometer. A limitation of our study is that we had a small sample size in men as compared with women. We collected volunteer subjects, which obtained an unequal sample size by sex. Further studies are needed to determine whether our findings are consistent with a different race, sex and age groups. Another limitation of our study is that we were unable to adjust the joint angle or the effect of gravity in measuring the HHD, which may overestimate the leg strength.
In conclusion, we found that the HHD (microFET2) had good concurrent validity with interclass reliability in measuring leg muscle strength in healthy older adults aged 60 to 85 years. Public health agencies and clinicians should emphasize the importance of HHD in assessing leg muscle strength, as an alternative measure to the isokinetic dynamometer.
The author has no conflict of interest to disclose.
Leijendekkers, R. A., Hinte, G. V., Sman, A. D., Staal, J. B., Maria W. G. Nijhuis-Van Der Sanden, & Hoogeboom, T. J. (2017). Clinimetric properties of hip abduction strength measurements obtained using a hand-held dynamometer in individuals with a lower extremity amputation. Plos One, 12, e0179887.
Reinking, M. F., Bockrath-Pugliese, K., Worrell, T., Kegerreis, R. L., Miller-Sayers, K., & Farr, J. (1996). Assessment of quadriceps muscle performance by hand-held, isometric, and isokinetic dynamometry in patients with knee dysfunction. Journal of Orthopaedic & Sports Physical Therapy, 24, 154-159.