Associations among perfectionism, anxiety, and psychological well-being/ill-being in college athletes of South Korea
International Journal of Applied Sports Sciences, Vol.32, No.2, pp.75-83
https://doi.org/10.24985/ijass.2020.32.2.75
© Korea Institute of Sport Science
초록
The study was to investigate the relationships between perfectionism (i.e., self-oriented and socially-prescribed perfectionism) and psychological well-being (i.e., vitality)/ill-being (i.e., emotional/physical exhaustion) and to examine the mediating effects of competitive state anxiety on the relationships. Three hundred two collegiate athletes participated in the study (Mage = 21.12yrs, SD = 1.28). The participants completed four questionnaires: Multidimensional Perfectionism Scale, Revised Competitive State Anxiety Inventory-2, Subjective Vitality Scale, and Emotional/Physical Exhaustion from Athlete Burnout Questionnaire. The hypothesized model presented an acceptable fit to the data. Specifically, χ2 (80) = 179.99 (p < 0.001), CFI = 0.973, TLI = 0.965, SRMR = 0.042, and RMSEA = 0.052 with 90% CI [0.042, 0.062]. The results indicated that self-oriented perfectionism was negatively related to competitive state anxiety (β = -.14, p < .005) and positively related to vitality (β =.26, p < .001), whereas socially-prescribed perfectionism was positively related to competitive state anxiety (β =.28, p < .001) and emotional/physical exhaustion (β =.15, p < .05). Competitive state anxiety was negatively related to vitality (β = -.14, p < .05) and positively related to emotional/physical exhaustion (β =.31, p < .001). Competitive state anxiety partially mediated the relationships between socially-prescribed perfectionism and emotional/physical exhaustion. The full mediating effects of anxiety on the relationships between self-oriented perfectionism and emotional/physical exhaustion and between socially-prescribed perfectionism and vitality were observed. Findings supported that self-oriented perfectionism was functionally adaptive to and socially-prescribed perfectionism was maladaptive to athletes’ psychological well-/ill-being.
Abstract
The study was to investigate the relationships between perfectionism (i.e., self-oriented and socially-prescribed perfectionism) and psychological well-being (i.e., vitality)/ill-being (i.e., emotional/physical exhaustion) and to examine the mediating effects of competitive state anxiety on the relationships. Three hundred two collegiate athletes participated in the study (Mage = 21.12yrs, SD = 1.28). The participants completed four questionnaires: Multidimensional Perfectionism Scale, Revised Competitive State Anxiety Inventory-2, Subjective Vitality Scale, and Emotional/Physical Exhaustion from Athlete Burnout Questionnaire. The hypothesized model presented an acceptable fit to the data. Specifically, χ2 (80) = 179.99 (p < 0.001), CFI = 0.973, TLI = 0.965, SRMR = 0.042, and RMSEA = 0.052 with 90% CI [0.042, 0.062]. The results indicated that self-oriented perfectionism was negatively related to competitive state anxiety (β = -.14, p < .005) and positively related to vitality (β =.26, p < .001), whereas socially-prescribed perfectionism was positively related to competitive state anxiety (β =.28, p < .001) and emotional/physical exhaustion (β =.15, p < .05). Competitive state anxiety was negatively related to vitality (β = -.14, p < .05) and positively related to emotional/physical exhaustion (β =.31, p < .001). Competitive state anxiety partially mediated the relationships between socially-prescribed perfectionism and emotional/physical exhaustion. The full mediating effects of anxiety on the relationships between self-oriented perfectionism and emotional/physical exhaustion and between socially-prescribed perfectionism and vitality were observed. Findings supported that self-oriented perfectionism was functionally adaptive to and socially-prescribed perfectionism was maladaptive to athletes’ psychological well-/ill-being.
Introduction
Perfectionism as a personality trait is a multidimensional construct considered a person’s striving for flawless and achieving goals to meet excessively high standards while being hypercritical of own performance. Perfectionism comprises self-oriented perfectionism as a personal component and socially prescribed perfectionism as a social component (Hewitt et al. 1991). Self-oriented perfectionism is defined as “unrealistic standards and perfectionistic motivation for the self,” whereas the socially prescribed perfectionism is defined as “the belief that significant others expect oneself to be perfect” (p. 464, Hewitt et al., 1991). One with more self-oriented perfectionistic tendency sets and has high (or often unrealistic) standards for one and drive one to be perfect and attain the standards. One’s perfectionistic behaviors are directly related to oneself. However, one with more socially prescribed perfectionistic tendency believes that others (e.g., parents and coaches) already set standards/goals for one and expect one to be perfect and attain the standards. Because one tries to be perfect, meet others’ expectations, and make other satisfied, it is an important notion that one’s perfectionistic behaviors are directly connected with others and that gaining others’ approval and acceptance is most crucial for those who have socially prescribed perfectionism.
The concept and description of perfectionism, as aforementioned, has been accepted and used in the sports field. Athletes practice numerous hours not to make unacceptable mistakes during games, and this perfectionistic tendency is considered a key characteristic for athletes to achieve elite performance and succeed in their sports (Gould et al., 2002). Research has shown perfectionism tendency was associated with psychological well-being and ill-being in athletes (Gaudreau & Verner-Filion, 2012; Hill & Curran, 2016). For example, self-oriented perfectionism was related to vitality, positive affect, and life satisfaction, whereas socially prescribed perfectionism was associated with burnout.
Athletes in competitive sports have performance-related stress (Li et al., 2019), and anxiety, an individual reaction to a stressful situation, has been of interest in the sport science field. The competitive sport can become a highly anxiety-provoking environment for athletes because winning is always a priority. Competitive state anxiety is an immediate and sport situation-specific multidimensional construct that comprises three dimensions: cognitive anxiety, somatic anxiety, and self-confidence (Martens et al., 1990). Both cognitive anxiety and self-confidence are intimately related to mental aspects of anxiety caused by self-evaluation/criticism and negative expectations about success or by fear of failure; however, somatic anxiety is the physiological and affective aspects of anxiety directly influenced by autonomic arousal (Martens et al., 1990). Anxiety research in sports has shown that anxiety had significant relations with performance, psychological ill-being (e.g., burnout and depression), and injury (Cohen et al., 2014; Cremades et al., 2011; Jensen et al., 2018; Lavallée & Flint, 1991).
Research has also shown significant relationships between perfectionism and competitive anxiety in athletes (Hill et al., 2018; Stoeber et al., 2007). Perfectionism was positively correlated with competitive anxiety, whereas it was negatively related to self-confidence. Specifically, fear of failure and worry about mistakes had positive correlations with cognitive anxiety and negative correlations with self-confidence. It shouldn’t be surprising that negative reactions to imperfection could be interpreted as anxiety. Intriguingly, personal standards had no significant correlation with competitive anxiety.
It can be expected that anxiety is closely associated with psychological well-being/ill-being in that as aforementioned, athletes in competitive sports have a great deal of excessive stress. Studies have reported that anxiety could be a strong predictor of psychological ill-being in athletes because the feeling of frustration, lack of confidence, and concentration problems as common anxiety symptoms (e.g., lack of confidence and worry about failure) were intimately related to emotional and physical exhaustion (Gustafsson et al., 2008; Cremades et al., 2011).
In sum, from the results of previous research, some correlations and causal relationships were revealed among perfectionism, anxiety, psychological well-being/ill-being in collegiate athletes. However, research on investigating causal relationships among them simultaneously is still limited. Therefore, the purpose of this research note was to investigate the relationship between perfectionism and psychological well-being/ill-being and to examine the mediating effects on the relationship.
Methods
Participants
A total of 302 collegiate athletes (238 males and 64 females) from 3 southern universities in the U.S. participated in the study. The subjects participated in various sports, including baseball, basketball, golf, softball, and soccer. The participants’ ages ranged from 20 to 25 years old, and the mean age was 21.12 years with SD = 1.28 years. The participants were in pre-season.
Measures
Perfectionism. The short version of the Multidimensional Perfectionism Scale (Hewitt & Flett, 1991) was used to assess athletes’ self-oriented perfectionism (SOP; e.g., “I must work to my full potential at all times”) and socially prescribed perfectionism (SPP; e.g., “The people around me expect me to succeed at everything I do”). This scale contains 10 items (5 items in each dimension) measured using a 5-point Likert scale ranging from 1 (not at all) to 5 (very much).
Competitive State Anxiety. The Revised Competitive State Anxiety Inventory-2 (CSAI-2R; Cox et al., 2003) was used to measure athletes’ state anxiety response to competitive sport situations. It contains 17 items: somatic anxiety (5 items; e.g., “My body feels tense”), cognitive anxiety (7 items; e.g., “I am concerned that I may not do as well in this competition as I could”), and self-confidence (5 items; e.g., “I'm confident about performing well”). The 17 items were measured on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much so).
Psychological Well-Being. The Subjective Vitality Scale (SVS; Ryan & Frederick, 1997) was used to assess the athletes’ subjective feelings of vitality (e.g., “I look forward to each new day”). The scale contains the 7 items measured on a 5-point Likert scale ranging from 1 (not at all) to 5 (very much).
Psychological Ill-Being. Consistent with previous research (Quested & Duda, 2009), the emotional/physical exhaustion subscale from Athlete Burnout Questionnaire (EPE; Raedeke & Smith, 2001) was used to measure athletes’ psychological ill-being (e.g., “I am exhausted by the mental and physical demands of [my sport]”). It contains 5 items measured on a 5-point Likert scale ranging from 1 (almost never) to 5 (almost always).
Procedures
After obtaining the Institutional Review Board (IRB) approval, the authors contacted coaches of collegiate sport teams, explained the purpose of this study, and asked their permission to visit their practice sites in order to recruit participants (i.e., student-athletes). With coaches’ permission, the authors visited their practice sites before or after their practice sessions. The coaches first introduced the authors to the athletes and left the sites. The authors explained the purpose of this study and informed that their participation was voluntary and anonymous and that they could withdraw from the participation without penalty. They were told to ask any questions before, during, and after completing the series of questionnaires. After signing the consent form and completing the survey, the athletes put the survey into an envelope and left the sites.
Data Analysis
Among 346 collegiate athletes with informed consent, 338 athletes completed the series of questionnaires (the response rate was 97.69%); however, 36 incomplete responses were excluded. Therefore, the data completed by 302 athletes were analyzed for this study.
Descriptive statistics, univariate skewness, univariate kurtosis, and correlations were calculated using the Statistical Package of the Social Sciences (SPSS 25.0). The cut-off criteria of the univariate normality assumption were absolute values of 2 for skewness and 7 for kurtosis. Additionally, Mplus 7 was used to conduct the structural equation modeling (SEM) to examine the full structural model, and parceling strategies were used to increase the stability of the parameter estimates (Little et al., 2002). First, construct-specific parcels were created for the CSAI-2R. That is, the three subscales (i.e., cognitive anxiety, somatic anxiety, and self-confidence) in the CSAI-2R were used as indicators. For example, cognitive anxiety was used as one of three indicators for the CSAI-2R. Second, item parcels were created for the SOP, SPP, SVS, and EPE. For items to construct balance, a stronger loading item was paired with a weaker loading item within a subscale (Little et al., 2002).
The two-step approach suggested by Anderson and Gerbing (1988) was used to evaluate the full structural model, including a measurement model and a structural model. The measurement model was assessed to examine the psychometric properties of the measures as well as the relationships between latent variables and their indicator variables, whereas the structural model was assessed to evaluate the causal relationships between latent variables. For the mediating effect analysis, 2,000 bootstrap samples were utilized. The chi-square (χ2) test, Comparative Fit Index (CFI), and Tucker-Lewis Index (TLI), standardized root mean square residual (SRMR), and root mean square error of approximation (RMSEA) were used to evaluate the overall fit of the measurement model and of the structural model. Cut-off points of below. 08 for RMSEA, below .08 for SRMR, and above .95 for CFI and TLI were considered acceptable. Construct reliability (CR) and average variance extracted (AVE) were calculated. The suggested cut-off points of the CR and AVE values were .7 and .5, respectively (Hair et al., 2010).
Results
Descriptive Statistics
Table 1 shows the means and standard deviations. All variables indicated satisfactory univariate skewness and kurtosis. That is, the overall values of skewness and kurtosis ranged from -.38 to .30 and from -.66 to -.15, respectively, and thus, the univariate normality was supported in that the absolute value of each item’s skewness was below 2 and kurtosis was below 7.
Table 1.
Means (M), standard deviation (SD), skewness, kurtosis, and correlations of scales.
| M | SD | Skewness | Kurtosis | |
|---|---|---|---|---|
| Self-oriented perfectionism | 3.55 | .91 | -.38 | -.15 |
| Socially prescribed perfectionism | 2.94 | 1.03 | -.12 | -.53 |
| Competitive state anxiety | 2.06 | .65 | .30 | -.66 |
| Psychological well-being | 4.76 | 1.37 | -.15 | -.48 |
| Psychological ill-being | 2.87 | .83 | -.13 | -.46 |
Table 2.
Factor correlations, composite reliability (CR), and average variance extracted (AVE)among the variables
| SOP | SPP | CSAI-2R | SVS | CR | AVE | |
|---|---|---|---|---|---|---|
| SOP | - | .90 | .74 | |||
| SPP | .31*** | - | .87 | .69 | ||
| CSAI-2R | -.06 | .24*** | - | .84 | .64 | |
| SVS | .27*** | .08 | -.15* | - | .92 | .78 |
| EPE | -.07 | .19** | .35*** | -.25*** | .76 | .53 |
Measurement Model
The fit indices for the measurement model were χ2 (80) = 164.43 (p < 0.001), CFI = 0.973, TLI = 0.964, SRMR = 0.042, and RMSEA = 0.042 with 90% CI [0.037, 0.058]. The overall fit of the measurement model was acceptable. Standardized factor loading values of all items within the measurement model ranged from 0.522 to 0.943. The values of the CR ranging from 0.76 to 0.92 and AVE values ranging from 0.53 to 0.78 were above the suggested cut-off points of 0.06 and 0.05, respectively (Fornell & Lacker, 1981). The values of the standardized factor loading, CR, and AVE provided evidence for satisfactory convergent validity and internal consistency.
Table 3.
Standardized path coefficients for the structural model
| Hypothesized Path | β | |
|---|---|---|
| Direct | Indirect | |
| Self-oriented perfectionism → competitive anxiety | -.14** | |
| Self-oriented perfectionism → psychological well-being | .26*** | |
| Self-oriented perfectionism → psychological ill-being | -.10 | |
| Socially prescried perfectionism → competitive anxiety | .28*** | |
| Socially prescried perfectionism → psychological well-being | .03 | |
| Socially prescried perfectionism → psychological ill-being | .15* | |
| competitive anxiety → psychological well-being | -.14* | |
| competitive anxiety → psychological ill-being | .31*** | |
| Self-oriented perfectionism → competitive anxiety → psychological well-being | .02 | |
| Self-oriented perfectionism → competitive anxiety → psychological ill-being | -.04* | |
| Socially prescried perfectionism → competitive anxiety → Psychological well-being | -.04** | |
| Socially prescried perfectionism → competitive anxiety → Psychological ill-being | .09* | |
Structural Model
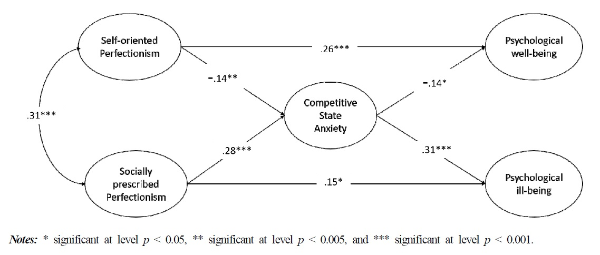
We tested the structural model. Figure 1 shows the results of the path coefficients among the subscales. The fit indices for the structural model were χ2 (80) = 179.99 (p < 0.001), CFI = 0.973, TLI = 0.965, SRMR = 0.042, and RMSEA = 0.052 with 90% CI [0.042, 0.062]. The overall model fit of the structural model was acceptable. As indicated in Figure 1, both self-oriented perfectionisman (β = -.14, p < .005) and socially prescribed perfectionism (β = .28, p < .001) significantly influenced compatitive state anxiety. Anxiety also significantly influenced psychological well-being (β = -.14, p < .05) and psychological ill-being (β = .31, p < .001) were also significant. The direct effect from self-oriented perfectionism to psychological well-being was significant (β = .26, p < .001), whereas the direct effect from socially prescribed perfection to psychological ill-being was significant (β = .15, p < .05). The bootstrapping results indicated that there were full mediating effects from self-oriented perfectionism to psychological ill-being via anxiety (β = -.04, p < .05) and from socially prescribed perfectionism to psychological well-being via anxiety (β = -.04, p < .05). There was also a partial mediating effect from socially prescribed perfectionism to psychological ill-being via anxiety (β = .09, p < .001).
Figure 1.
Structural equation model with standardized estimates in the relations between self-oriented perfectionism, socially prescribed perfectionism, competitive anxiety, psychological well-being, and psychological ill-being. Only significant paths are presented.
Discussion
The purpose of this research note was to examine the relationship between perfectionism, competitive state anxiety, and psychological well-being/ill-being. Specifically, we aimed to investigate the mediating effects of competitive state anxiety on the relationship between perfectionism and psychological well-being/ill-being in collegiate athletes.
First, self-oriented perfectionism had a significant path to psychological well-being (β = .26, p < .001), whereas socially prescribed perfectionism had a significant path to psychological ill-being (β = .15, p < .05). These results supported that different types of perfectionism have different functions (Dunn et al., 2006; Stoeber & Otto, 2006). As an adaptive function, self-oriented perfectionism was considered perfectionistic strivings (e.g., a self-oriented striving to meet high standards set by one and to be excellent) and associated with vitality, conscientiousness, emotional adjustment, positive affect, excellence, and life satisfaction (Gaudreau & Verner-Filion, 2012; Gould et al., 2002; Hill & Curran, 2016; Hill et al., 1997). On the other hand, as a maladaptive function, socially prescribed perfectionism was considered perfectionistic concerns (e.g., concerns to be perfect to meet others’ expectations).
Socially prescribed perfectionism had a significant path to competitive state anxiety (β = .28, p < .001), and the result supported previous research indicating that this type of perfectionism was related to negative characteristics and emotions more than positive ones (Dunn et al., 2006; Hill & Curran, 2016; Stoeber et al., 2007). As defining socially prescribed perfectionism (Hewitt & Flett, 1991), some athletes in competitive sports may push themselves to be perfect and meet others’ expectations, and they can have feelings of fear of failure to meet others’ expectations and of reaction to imperfection. The feelings are in line with anxiety characterized by negative expectations and consequences and thus can increase feelings of anxiety in sport situations. Self-oriented perfectionism was significant predictive of competitive anxiety (β = -.14, p < .005). This result supported that as aforementioned, self-oriented perfection has a positive and adaptive function to have higher levels of self-confidence and lower levels of cognitive and somatic anxiety in athletes (Hamidi, & Besharat, 2010).
Competitive state anxiety had significant paths to psychological well-being (β = -.14, p < .05) and psychological ill-being (β = .31, p < .001). The result supported previous research finding that anxiety is strongly correlated with psychological ill-being (Cho et al., 2019; Cohen et al., 2014). For example, the higher levels of anxiety were related to the risk of burnout in athletes (Goodger et al., 2007). Although competitive state anxiety is characterized by a feeling of anxiety to a sport-specific situation at an immediate moment, when athletes repeatedly face the same situation, the feeling of anxiety can cause more severe psychological and mental health issues such as burnout and depression.
The mediation results, again, supported that self-oriented perfectionism has a healthy and adaptive function and socially prescribe perfectionism has a maladaptive function. That is, specifically, self-oriented perfectionism negatively influenced competitive state anxiety that was positively predictive of psychological ill-being. Socially prescribed perfectionism positively influenced competitive state anxiety that was negatively predictive of psychological well-being and positively predictive of psychological ill-being. The results support that socially prescribed perfectionism as perfectionistic concerns had a strong indirect effect on psychological ill-being via competitive anxiety (Jensen et al., 2018).
There are limitations to generalize the current findings. First, a cross-sectional design used to collect the data in this study is limited to provide clear causal relationships between variables. Competitive state anxiety changes 1 day, hours before, 30 minutes, and during competitions. It is even different in and off-season. Collegiate athletes may feel more physically and mentally exhausted because they have to well maintain their dual roles (i.e., as a student and as an athlete). Therefore, a longitudinal study design should be used to confirm the causal relationships between perfectionism, competitive state anxiety, and psychological well-being/ill-being in collegiate athletes. A recent meta-analysis study has shown type of sport (e.g., team sport vs. individual sport) and type of skill (e.g., open skill vs. open skill) were moderator variables of the competitive state anxiety. However, this current study didn’t specify moderator variables for the competitive state anxiety. For future research, the multi-group comparison using SEM should be guaranteed to clearly provide causal relations.
The results of this study provide practical information for coaches, parents, and mental performance consultants. Perfectionism is multidimensional, but not dichotomous. An athlete in competitive sports can strive him/herself to meet a high standard/goal which was set by him/herself and at the same time to meet others’ expectations (e.g., parents expect the athlete to place first at the upcoming regional swimming competition). If the athlete perceives that wining is more important than improving personal performance (i.e., socially prescribed perfection is emphasized), “have to win” mind weighs on the athlete, and he/she may have a fear of failure (i.e., not to meet others’ expectations) and worry about negative outcomes and imperfection and in turn have higher levels of anxiety and psychological ill-being. Self-oriented perfectionism may help the athletes control and manage the competitive sport situations, reduce their competitive anxiety, and consequently improve psychological well-being.