Low volume progressive single set of resistance training is as effective as high volume multiple sets of resistance protocol on muscle strength and power.
International Journal of Applied Sports Sciences, Vol.27, No.1, pp.33-42
ⓒ Korea Institute of Sport Science
초록
The purpose of this study was to compare the effects of traditional high volume multiple set resistance training and low volume progressive single set training on muscular strength and power in healthy male college students. A total of 19 students were randomly assigned to either a single set (ST, n=6), multiple sets (MT, n=7), or control group (CON, n=6). The ST (every 3rd day, 50-100% of 1RM, maximum 8 reps, single set) and MT (3 times/week, 70% of 1RM, 10 reps with 3 sets) trained for 8 weeks using an inclined leg press. One-repetition maximum (1RM), muscle maximal voluntary contraction, peak power, and electromyography were measured at baseline and after 8 weeks of training. Repeated-measured ANOVAs were used to find interaction effect between trial and treatment group factors. There was no significant increase on peak power after 8 weeks of resistance training both in MT (p = .286) or ST (p = .372). 1RM in both training groups was significantly increased compared to their baseline values (p < .001). However, there was no significant difference in 1RM between the two training groups after 8 weeks of training. It indicates that ST is as effective as traditional high volume multi sets training protocol (MT) for increasing muscle strength.
Abstract
The purpose of this study was to compare the effects of traditional high volume multiple set resistance training and low volume progressive single set training on muscular strength and power in healthy male college students. A total of 19 students were randomly assigned to either a single set (ST, n=6), multiple sets (MT, n=7), or control group (CON, n=6). The ST (every 3rd day, 50-100% of 1RM, maximum 8 reps, single set) and MT (3 times/week, 70% of 1RM, 10 reps with 3 sets) trained for 8 weeks using an inclined leg press. One-repetition maximum (1RM), muscle maximal voluntary contraction, peak power, and electromyography were measured at baseline and after 8 weeks of training. Repeated-measured ANOVAs were used to find interaction effect between trial and treatment group factors. There was no significant increase on peak power after 8 weeks of resistance training both in MT (p = .286) or ST (p = .372). 1RM in both training groups was significantly increased compared to their baseline values (p < .001). However, there was no significant difference in 1RM between the two training groups after 8 weeks of training. It indicates that ST is as effective as traditional high volume multi sets training protocol (MT) for increasing muscle strength.
Introduction
Resistance training is known for inducing muscle hypertrophy (increase in muscle size), increasing maximum muscle strength and endurance, and for improving physical performance, while preventing or attenuating age-related muscle atrophy (ACSM, 2009; Lee & Farrar, 2003). An alteration of hormone levels, increasing neuromuscular activity, and development of muscle motor unit recruitment, as well as change in muscle hypertrophic protein concentration are results of physical adaptation by resistance training (Kraemer et al., 2002).
The key determinants for inducing muscle hypertrophy and improving muscle strength are resistance training volume and intensity. Various resistance training programs require a different volume of training with variations of frequency, intensity, and duration of the exercise in each session. Different types of resistance training protocols have been extensively studied for half a century. Early resistance training protocols generally assumed a minimum of three sets of 7-10 repetitions of each exercise provided the greatest gains in muscle strength and mass (ACSM, 2009). According to the American College Sports Medicine (ACSM, 2013), 2-4 sets of 8-15 repetitions is the recommended protocol for general and athletic populations. In healthy and well-trained populations, multiple sets of resistance training have been shown to achieve maximum muscle strength (Carpinelli & Otto, 1998) whereas single set training has been shown to be effective in untrained individuals (Baker et al., 2013; Tan et al., 2014).
However, researchers challenged the assumption made in 1990’s that multiple sets are more effective than a single set, when studies showed single sets may be just as effective as multiple sets (Krieger, 2010). Although many studies compared the effectiveness of a single set to multiple sets for muscle strength and mass increase (Backer et al., 2013; Cameron et al., 2012; Krieger, 2010; Mark et al., 2013), controversial research findings have yet to conclusively determine whether either protocol is more effective than the other (Frohlich, Emrich, & Schmidtbleicher, 2010).
One study comparing single versus multiple sets of resistance training on muscle strength and body composition demonstrated that single sets of high-intensity resistance training is as effective as multiple sets to increase upper-body muscle strength (Backer et al., 2013; Abrahin et al., 2014). Furthermore, a study investigated three levels of resistance training intensity and volume measured isometric muscle strength and muscle hypertrophic markers to compare the effectiveness of the training protocols (Cameron et al., 2012). The study reported that the single set and multi sets increased the isometric muscle strength and muscle hypertrophic markers with no significant difference among groups. However, this result conflicts with an earlier meta-analysis study (Krieger, 2010), which claimed multiple sets of resistance training is more effective on muscle strength and muscle hypertrophy compared to single set of resistance training.
We recently developed low volume progressive high intensity single set resistance training protocol and demonstrated similar hypertrophy responses to the traditional high volume multiple sets training protocol in animal model (unpublished data). So, we wanted to test this new protocol for human model. The purpose of this study is to evaluate and compare the effects of traditional high volume multiple set resistance training and low volume progressive single set training on muscular strength and power in healthy male college students.
Methods
Participants
This study was approved by the Texas A&M University-San Antonio Institutional Review Board (IRB) for testing on human subjects. Nineteen healthy young men (22-32 yr) voluntarily participated in this study. Before signing the consent form, they were explained the detailed procedure for the research project and informed of the procedure and potential risks involved in the investigation. Subjects were excluded from this study if they were suffering from an injury or musculoskeletal limitations that might affect subject’s ability to participate for this study. Furthermore, subjects were required to have completed at least 80% of the training session in order to be included for data analysis. The subjects were randomly assigned to either the single set (ST, n=6), multiple set (MT, n=7), or control group (CON, n=6), described in table 1.
Table 1.
Subjects characteristics
| CON (n = 6) | ST (n = 6) | MT (n = 7) | |
|---|---|---|---|
| Age (yrs) | 25.67 ± 3.72 | 27.62 ± 3.83 | 28.57 ± 4.47 |
| Weight (kg) | 86.53 ± 15.88 | 98.14 ± 11.99 | 89.28 ± 15.82 |
| Height (cm) | 173.34 ± 3.83 | 172.90 ± 5.22 | 177.53 ± 8.30 |
| %Body fat | 29.75 ± 5.56 | 29.93 ± 3.94 | 24.57 ± 8.04 |
Anthropometrics
Height was measured using a wall stadiometer (PAT#290237, Novel Products, Rockton, IL, USA) and body weight was measured using Health O meter (HJF-400, Bridgeview, USA). Body fat was measured by bioelectrical impedance analysis using Omron (HBF-510W, Kyoto, Japan) by having a subject stand on a monitor with no shoes or socks and no metal objects attached to their body.
Resistance Training Protocol
The RT protocol was applied over an 8-week period. Prior to training, all subjects had their 1 repetition maximum (1RM) assessed in order to determine their initial weight for resistance training. One RM was measured using direct method. Briefly, after a warm up, subjects selected a weight that is achievable. Then after a rest of at least several minutes, subjects increased the weight and tried again. The subjects selected subsequent weights until they can only repeat one full and correct lift of that weight. The MT consisted of 3 sets of 10 repetitions with 70% of 1RM 3 times per week for 8 weeks, with a two-minute rest interval between the sets. The subjects in ST trained once a day every third day (1st, 4th, 7th, etc) for eight weeks. Therefore, they trained 2 to 3 times per week depending on weekly schedule. On the first day, ST subjects were trained with 6 repetitions using 70%, 75%, 80%, 85%, 90% and 100 % of their 1RM. After the first day of training, the training protocol consisted of 50%, 75%, 90%, and 100% of previous maximal loads for the first four repetitions. After first four repetitions, 10 lb was added to each rep until a new 1RM was achieved (table 2). If they failed to lift a weight at any time of during the training, the weight was set to the previous maximum weight for the next repetition. Research assistants were present during all training session to assist and to supervise resistance training and for safety.
Table 2.
Resistance protocol for single set training
| Reps | First day of training | Reps | Protocol (After first day of training) |
|---|---|---|---|
| 1 rep | 70% of their 1RM | 1 rep | 50% of previous max |
| 2 rep | 75% of their 1RM | 2 rep | 75% of previous max |
| 3 rep | 80% of their 1RM | 3 rep | 90% of previous max |
| 4 rep | 85% of their 1RM | 4 rep | 100% of previous max |
| 5 rep | 90% of their 1RM | 5 rep | 4thweight+10lb |
| 6 rep | 100% of their 1RM | 6 rep | 5thweight+10lb |
| 7 rep | 6thweight+10lb | ||
| 8 rep | 7thweight+10lb |
Maximum Isometric Strength Measurement
Maximal voluntary contraction (MVC) of the knee extension in dominant leg was performed on an isokinetic dynamometer (Cybex Orthotron, CSMI, USA) to determine isometric muscle strength. All subjects underwent five minutes of a warm-up period that consisted of stretching exercise for their lower legs and familiarization trail, which consisted of three 5-sec unilateral isometric contractions. Subjects sat on the Cybex Orthotron with arms crossed and their leg was firmly strapped to the seat with knee angle set at 90°. The rotational axis of the dynamometer was adjusted to the lateral femoral epicondyle and the lower leg was attached to the dynamometer lever arm above the medial malleolus, with no static fixation of the ankle joint. On the signal from the investigator, subjects kicked the dynamometer lever arm as hard as they could. The same backrest setting, dynamometer head setting, and lever arm length were used for pre and post training for each subject. Subjects performed three trials with one minute break between each trail, with the highest MVC recorded and reported.
Electromyography (EMG)
Muscular electrical activity was measured for all subjects using iWorx (IX-TA-220, Dover, USA). Muscle electrical signals were recorded from vastus lateralis of the dominant leg while measuring the MVC during leg extension exercise. Five electrodes were placed on the leg with one electrode placed on the end of the VL (above the knee) and the second one placed 10 cm higher than previous point. The third one was placed on the bottom of hamstring and fourth one was placed 10 cm superior of that point. The last electrode was placed on the lateral malleolus. At each site where the electrode was placed, the skin was shaved, abraded, and cleaned with alcohol wipes. All data were recorded and analyzed by LabScribe3 software (iWorx, Dover, USA). The EMG signals were amplified and filtered to reduce noises using pre-installed software. Briefly, LabScribe3 software program applies a user-controlled FIR (Finite Impulse Response) filter. The cutoff frequency is user-selected - a single or dual pass filter is applied to the envelope to generate the individual plots allowing the graphs to be generated with typical data processing delays for comparison with older data, or with delay free results for current research. It can generate a graph of raw EMG for each recorded EMG channel. Graphs can be scaled by %, or surface potential display full leg contraction during the leg extension. "Normal" EMG activity bars were displayed and printed and each EMG graph labeled with a muscle name. The maximal of muscle activity value (mV) was reported.
The Wingate Test
Anaerobic power was measured by a 30 sec Wingate test on a Monark cycle ergometer (894E, Varberg, Sweden) using 0.09kp per kg body mass. The subjects for this study were all healthy young Kinesiology major. So, we calculated load based on equation for active people (0.09kp per kg body mass) not sedentary (0.075kp per kg body mass).
Warm-up consisted of lightly pedaling for 40-45 seconds without resistance, followed by three 5-sec sprints using a predetermined resistance. Upon completion of the warm-up, subjects rested for two minutes before the 30 sec Wingate test. Just prior to the start of the Wingate test, the subjects pedaled progressively faster without resistance for 10 sec, at which time they were pedaling at maximal RPM. At this point the resistance pan was released and the subject countinued to pedal at maximal effort for 30 seconds. Every five seconds RPM were counted and recorded. Once 30 seconds was completed, the subject pedaled without resistance in a cool-down phase for 3 minutes.
Statistics
All statistical analyses were conducted using SPSS 20.0 (SPSS inc, Chicago, USA). Descriptive statistics including mean and standard deviation were computed for whole group and sub-groups. 3 (group) × 2 (trial) repeated-measure ANOVAs were used to determine an interaction effects between trial and treatment groups factors for each dependent variable. If an interaction was significant, differences were examined with pairwise comparisons. Main effects were explored to determine pre and post differences by different groups. The LSD post hoc test procedure was used to identify which groups were significantly different. Statistical significance was accepted for repeated-measure ANOVAs tests at p < .0125 and pairwise comparison was set at p < .05.
Results
One Repetition Maximum
There was significant interaction effect for 1RM between trials and treatment group factors, F (2, 15) = 11.15 p = .001. Pairwise comparison revealed a significant change of the 1RM difference between the pre and post time points, (p = .000) in which the ST and MT significantly increased 1RM compared to the baseline after the 8-week resistance training. 1RM was significantly increased in all training groups compared with CON (p < .05), but there was no significant difference between ST and MT in 1RM after 8-weeks of resistance training (figure 1). Therefore, this result indicates that low volume progressive single set resistance training is as effect as traditional high volume multiple sets resistance training.
Maximal Voluntary Isometric Contraction
There was a significant interaction effect for maximal voluntary isometric contraction (MVC) between trials and treatment group factors, F (2, 15) = 14.94 p = .000. Pairwise comparison revealed a significant difference on MVC between pre and post time points in MT (p = .000), but not in ST (p = .089). There was no significant difference between the pre- and post- MVCs in the CON (p = .814), (table 3). In addition, there was a significant difference in MVC between CON and MT (p = .044), but not between ST and MT (p = .918) after 8-weeks of resistance training (table 3).
Fig 1.
Values are presented as means±SD (lb); CON: Control group, ST: Single set training group, MT: Multi sets training group, *Significant difference between pre- and post-test (p < .05), #Significant difference between treatment groups and control group (p < .05).
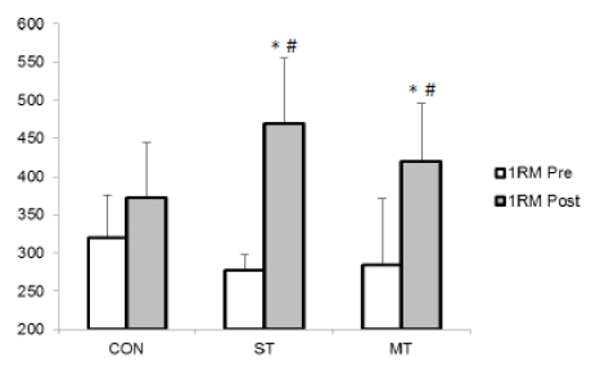
Table 3.
Changes in MVC after 8-week resistance training
Peak Power
There was no significant interaction effect between trials and treatment group factors on peak power (F (2, 15) = .056 p = .946). Pairwise comparison revealed no significant difference on peak power between pre and post time points for the ST (p = .372) and MT (p = .286) groups after 8-weeks of resistance training. There was no significant difference between the pre- and post-peak powers in the control group (p = .190) (table 4).
Table 4.
Changes in relative peak power after 8-week resistance training
| CON (n=6) | ST (n=6) | MT (n=7) | |
|---|---|---|---|
| Relative Peak Power Pre (w/kg) | 11.00 ± 2.10 | 11.80 ± 2.26 | 11.18 ± 3.79 |
| Relative Peak Power Post (w/kg) | 12.17 ± 1.74 | 12.67 ± 1.18 | 12.06 ± 3.04 |
Electromyography
There was no significant interaction effect on EMG between trials and treatment group factors (F (2, 15) = .1.25 p = .312). Pairwise comparison revealed significant difference in EMG activity between pre and post time points for MT (p = .043), but not for ST (p=.206) and CON (p=.919) (table 5).
Table 5.
Changes in EMG activity after 8-week resistance training
| CON (n=6) | ST (n=6) | MT (n=7) | |
|---|---|---|---|
| EMG Pre (mv) | 5.41 ± 0.82 | 6.00 ± 0.95 | 4.36 ± 1.17 |
| EMG Post (mv) | 5.33 ± 1.64 | 7.00 ± 1.98 | 5.91 ± 1.41* |
Discussion
Since the 1960’s, a number of studies were conducted to determine an appropriate and effective resistance training protocol with various sets and repetitions to increase muscle strength and size (Lawrence, 1999; Krieger, 2010). Although many investigators have used different types of resistance training protocols (Cholewa et al., 2014; Frohlich, M., Emrich, E., & Schmidtbleicher, D, 2010), it is still debatable whether a high-volume or low-volume training protocol is preferable to induce muscular hypertrophy and increase muscle strength.
The purpose of this study was to evaluate and compare the multi-set resistance training protocol to a single set resistance training protocol in hopes of determining the optimal protocol for increasing muscle strength in healthy young men. Results indicate the 1RM value was significantly increased in both groups (ST and MT), however, there was no significant difference between ST and MT training groups in 1RM. The CON did not increase their 1RM after the 8 weeks and they were significantly lower than the ST and MT groups.
These results are consistent with previous studies, one of which reported that resistance training with 30% of 1RM-3 sets, 80% of 1RM-1 set, and 80% of 1RM-3 sets was not statistically different in 1RM change among three groups after 10 weeks of training (Mitchell & Breen, 2012; Abrahin et al., 2014). Another study also conducted low-volume circuit resistance training and high-volume resistance training to determine the long-term training adaptation after a 24-week training period (Marx et al., 2012; Tan et al., 2014). The 1RM bench press and leg press increased significantly in both low-volume and high volume of resistance training at 12-week compared with baseline, but only high-volume periodized resistance training increased at 24-week. In addition, this result showed that low-volume, single set training is as effective in maintenance of muscle strength as multi set training. The key finding from this study is that the low-volume of resistance training (single set training) with progressive weight produced similar effectiveness in improving strength as multi sets training measured by 1RM (Tan et al., 2014).
(Bemben et al. (2000) reported that 6-months of resistance training with lower repetition and higher intensity (80% of 1RM, 8 reps/3 sets) produced relatively similar and sufficient lower body muscle strength compared with higher repetition and lower intensity (40% of 1RM, 16 reps/3 sets). Even though resistance exercise with heavier load and higher volume has been accepted as a sufficient training protocol to increase muscle strength (McArdle, Katch & Katch, 2007), the results of this study partially support the positive effect of lower volume programs that may also produce greater compliance by reducing financial cost and time commitment rather than doing high volume of exercise.
There was a significant difference between pre and post tests on MVC in MT training group only. This is contradictory to a previous finding in which MVC was significantly increased in both low-volume and high-volume of resistance training (Mark et al., 2001). However, single-set training in the previous study was conducted for 24 weeks and had more total volume of resistance training compared to 8 weeks of ST in current study. Therefore, the difference of total volume of resistance training may have caused this discrepancy in MVC compared to the previous study, suggesting more prolonged training is required to see the increase of MVC in ST.
Mitchell et al. (2001) also reported that three different resistance training protocols (80% of 1RM with one set, 80% of 1RM with three sets and 30% of 1RM with 3 sets) elicited the increase of MVC in all training condition with no between-condition differences. Lawrence et al. (1999) also conducted a study using with low (4 sets/3-5RM), moderate (4 sets/13-15RM), and high-repetition (4 sets/23-25RM) squats training three times per week for 7 weeks. The results indicated all training groups significantly increased MVC compared with baseline and CON and the low-repetition group improved more than did the high-repetition group. This result was able to support that resistance training at high intensity close to the maximum resistance (overload training) induce neuromuscular adaptation and increased muscle force development.
The findings of increased of MVC on both low-volume and high volume of resistance training in the previously cited studies underscored the effectiveness of low-volume, single set resistance training program, which is also effective in eliciting muscle strength gains. Although single set included a lower volume of exercise than multi sets of training, it showed similar muscle strength increases (Mitchell et al., 1985; Mark et al., 2001). However, our study demonstrated ST training did not show the significant increase compared with CON and baseline on MVC even though there was no significant difference between ST and MT on MVC. It is possible that a greater number of subjects is needed to elicit muscle strength gains in ST.
The Wingate test is used to assess anaerobic muscle power with peak power measured during the first 5-sec. From this study, there was no interaction effect for peak power between trials and groups in single set and multi set training group. Ormsbee et al. (2012) reported that 6-weeks of resistance training did not show time or group interaction effects on a peak power test in resistance-trained young men. In contrast, Beck et al. (2007) were able to find significant group and training effects for peak power after 10-week of resistance training. The major difference between Ormsbee et al. (2012) and Beck et al. (2007) was 6-week and 10-week of resistance training, respectively, which could be an effect factor for peak power. The current study may not have been long enough to induce changes in the muscle that would allow an increase in peak power to take place, similar to Ormsbee et al. (2012).
Mark et al. (2001) noted that the single set training did not significantly increase peak power compared with baseline, but multi sets training was sufficient to significantly increase peak power compared with baseline. The authors explained that the multi sets training group performed their repetitions with various contraction velocities and a diversity of training load. However, the single set training group performed each repetition in a controlled way. Traditionally, high velocity of resistance training has been known to be a more effective method to increase muscle power (Coyle et al., 1981), so it may be this rather than the number of sets that induced these differences.
In the present study, peak power in ST and MT resistance training was not significantly different compared with baseline and the CON. While the velocity of the repetitions may have contributed to this, it may also be due to short duration of resistance training and it is plausible that prolonged resistance training of more than 8 weeks might be required to elicit such a difference.
While there was no significant interaction among trials and groups for electromyography, it was significantly increased after eight weeks of RT compared with baseline in MT. Heavy-load RT influences recruitment of motor neurons and muscle fiber number, muscle size (hypertrophy), and muscle fiber composition (Aagaard, 2002). It is suggested that as muscle force increases, more motor neurons are progressively synchronized with muscle force (Gottlieb & Agarwal, 1971). Aagaard et al. (2002) used electromyography to show significant increase in force development and neural drive after 14 weeks of heavy-resistance training compared with baseline. These findings suggest that enhanced neural drive induced by resistance training increased electromyography signal and rate of electromyography development. Walker et al. (2011) examined EMG in eight healthy untrained men who performed a single contraction using three different RT protocols (increased resistance, reduced resistance, different knee angle). Electromyographic activity was significantly increased by increasing resistance during steady-paced contraction on vastus lateralis muscle.
The result of electromyography in present study supports the increase of muscular strength measured by 1RM on vastus lateralis muscle in multi sets training group after 8-week of resistance training. However, the reasons electromyographic activity in ST did not show the increase after 8-week of RT might be due to an insufficient stimulus to elicit such a difference.
There are several limitations for this study. Body mass index for CON and ST was 29.8 and 29.9, respectively. It is a border line between overweight and obese. Otherwise BMI for MT group is 24.6, which is normal healthy range. Even if there was no statistical difference on BMI between groups, it could be significant confounding factor. There was no direct measurement of muscle mass like girth and cross sectional area.
In summary, it was hypothesized there would be no significant difference in increase of muscle strength and power between MT and a ST after eight weeks of resistance training. There was a significant increase in 1RM after 8-weeks of training in both ST and MT groups; however, there was no statistical difference in 1RM between ST and MT group. MVC showed significant interaction effect between trials and groups, but there was only a significant difference on MVC in MT compared with baseline. Peak power did not show any significant changes on ST and MT group after 8-week of resistance training. Furthermore, there was no significant interaction effect on electromyography activity between trials and groups, but there was significant difference in electromyography on MT compared with baseline.
In conclusion, ST, a low volume progressive single set resistance training protocol is as effective as traditional high volume MT protocol for increasing muscle strength and power. This new single set training protocol could provide useful information for athletes and general public who want to maintain and/or improve their muscle strength wit relatively less time and efforts during the off season.
The authors thank Mr. Taylor Trevino for his excellent contribution on the data collection.
References
Baker, J. S., Davies, B., Cooper, S. M., Wong, D. P., Buchan, D. S., & Kilgore, L. (2013). Strength and body composition changes in recreationally strength-trained individuals: comparison of one versus three sets resistance-training programmes. Biomed Research International, 2013, 615901. doi: 10.1155/2013/615901
Beck, T. W., Housh, T. J., Johnson, G. O., Coburn, J. W., Malek, M. H., & Cramer, J. T. (2007). Effects of a drink containing creatine, amino acids, and protein combined with ten weeks of resistance training on body composition, strength, and anaerobic performance. Journal of Strength Conditioning and Research, 21(1), 100-104. doi: 10.1519/R-18685.1
Cameron J. Mitchell, Tyler A. Churchward-Venne, Daniel W. D. West, Nicholas A. Burd,, & Leigh Breen, Steven K. Baker, and Stuart M. Phillips. (2012). Resistance exercise load does not determine training-mediated hypertrophic gains in young men. Journal of Applied Physiology, 113, 71–77. doi: doi:10.1152/japplphysiol.00307
Cholewa, J., Guimaraes-Ferreira, L., da Silva Teixeira, T., Naimo, M. A., Zhi, X., de Sa, R. B., . . . Zanchi, N. E. (2014). Basic models modeling resistance training: an update for basic scientists interested in study skeletal muscle hypertrophy. Journal of Cell Physiology, 229(9), 1148-1156. doi: 10.1002/jcp.24542
Ormsbee, M. J., Mandler, W. K., Thomas, D. D., Ward, E. G., Kinsey, A. W., Simonavice, E., . . . Kim, J. S. (2012). The effects of six weeks of supplementation with multi-ingredient performance supplements and resistance training on anabolic hormones, body composition, strength, and power in resistance-trained men. Journal of International Society of Sports Nutrition, 9(1), 49. doi: 10.1186/1550-2783-9-49
Tan, J. G., Coburn, J. W., Brown, L. E., & Judelson, D. A. (2014). Effects of a single bout of lower-body aerobic exercise on muscle activation and performance during subsequent lower-and upper-body resistance exercise workouts. Journal of Strength Conditioning and Research, 28(5): 1235-40. doi: 10.1519/JSC. 0000000000000413