The development and validation of a rehabilitation capability questionnaire for injured athletes
Article information
Abstract
The purpose of this study was to develop and validate a Rehabilitation Capability Questionnaire (RCQ) that could measure the rehabilitation capabilities of injured athletes. A total of 240 injured athletes engaged in physical rehabilitation programs in Study 1 which followed a method proposed by Cohen, Montague, Nathanson, and Swerdik (1988). Fifty-two injured athletes who had been taking a physical rehabilitation program participated in Study 2. The convergent, discriminant, and predictive validities of the RCQ were analyzed. The results indicated that the RCQ retained four factors 22 items: emotional, cognitive, behavioral, and social support factors. The RCQ showed good, external validity.
Introduction
The Development and Validation of a Questionnaire for Assessing the Rehabilitation Capabilities of Injured Athletes
Maintaining a positive outlook during physical recovery and a strong desire to return to the field is the dominant, positive factors that aided in the successful recovery of injured athletes. Wiese-Bjornstal et al. (1998) proposed a model that depicts the importance of psychological factors and psychological responses to the rehabilitation process. This model indicated that pre-injury, personal and situational factors (Andersen & Williams, 1988) and post-injury consequences (Wiese-Bjornstal, Smith, & La Mott, 1995) affected an individual's psychological response. An athlete's psychological response could change dynamically over the course of the recovery period, and successful recovery is the desired outcome of the rehabilitation process. The model also suggests that when sports injury occur, psychological consequences, such as cognitive, emotional, and behavioral responses, and personal resources are important for the successful recovery of injured athletes.
Psychological factors and mediated variables (personal resources and social support) are considered very important variables for successful recovery. The previous studies (Shin, 2011; Wiese-Bjornstal et al., 1998) suggested that the rehabilitation capabilities of injured athletes are composed of psychological factors, behavioral factors, social support factors, and personal resource factors. Other factors that could mediate emotional responses, cognitive responses, behavioral responses, and successful recovery were injury history, recovery progress (McDonald & Hardy, 1990), general level of activity disruption (Crossman & Jamieson, 1985; Mainwaring, 1999), coping resources during injury rehabilitation (Udry, 1997), and perceived social support (Green & Weinberg, 2001; Udry, 1997). However, inventories that concurrently measure the rehabilitation capability of injured athletes are relatively sparse in the field of sports. Previous studies have frequently used the profile of mood state (POMS) questionnaire (McNair, Lorr, & Droppleman, 1971) to analyze the emotional responses of injured athletes (Shin & Yook, 2005). To assess cognitive responses to injury, research also uses the subjective injury estimation questionnaire (SISQ), which employs four dimensions (seriousness of the injury, interference with short-term and long-term expectations, and a fear of future relapses). Also, self-esteem questionnaires and self-efficacy questionnaires have been used to measure mental states of injured athletes. Questionnaires that assess the emotional states of injured athletes during recovery periods have never actually been used for research in the field of rehabilitation because these questionnaires have not been developed for injured athletes and could not measure the various psychology states and/or rehabilitation capabilities of injured athletes.
To assess the behavioral responses of injured athletes, such as their rehabilitation adherence level, a Rehabilitation Adherence Questionnaire (RAQ) can be used (Fisher, Domm, & Wuest, 1988). The RAQ is a self-inventory with subscales designed to assess the participation levels of injured athletes in rehabilitation programs. Despite consistency in the findings of studies using RAQs, particularly with respect to subscales for pain tolerance and support from significant others, research with the RAQs was limited in two important ways. First, because of their retrospective designs, the studies could not establish a time-order relationship between the psychological factors assessed by the RAQ and rehabilitation adherence. Second, because no reliability and validity data were reported for the RAQ, it could not be assumed that the RAQ subscales were stable, consistent measures or that they measured what they were intended to measure. The lack of confidence in RAQ findings, as described above, could not attract medical doctors and sport psychologists to rehabilitation centers (Shin et al., 2010).
Sports psychologists in rehabilitation center have traditionally used the Minnesota Multiphasic Personality Inventory (MMPI; Hathaway & McKinley, 1943) and its second edition, the Minnesota Multiphasic Personality Inventory-2 (MMPI-2; Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 1989) in psychological research and clinical practices that examined injured athletes. However, because the MMPI was not developed for injured athletes and experienced problems with response accuracy due to its many items (567 items), the validity of the MMPI decreased when applied to injured athletes. In light of this, it was necessary to develop a Rehabilitation Capability Questionnaire (RCQ) to measure the rehabilitation capability of injured athletes in the rehabilitation process. An RCQ should have not only internal, but also external, validity, and it should be used as a screening tool for medical and psychological healthcare providers. In other words, an RCQ must accurately diagnose the rehabilitation capability of injured athletes and the intervention effects from the onset of an injury until the end of recovery for their successful recovery. To address this, this study sought to examine the external validity, as well as the internal validity, of the RCQ developed in Study 1. The convergent validity, discriminant validity, and predictive validity of the RCQ were analyzed to test its validity.
Methods
Study 1
Participants
The participants in the study consisted of 240 injured athletes (exploratory factor analysis: 120, secondary analysis: 120) who participated in a physical rehabilitation program. The results of 120 injured athletes were utilized to conduct the descriptive statistics analysis, item analysis, and exploratory factor analysis. The results of another 120 injured athletes were utilized to conduct the confirmatory factor analysis to examine inter validity of the RCQ.
A total of 240 injured athletes (72% male, 28% female), from 13 to 25 years of age, participated in this study. These athletes were competing in international (5%), national (13%), provincial (40%), and regional (42%) events at the time of the study. The athletes participated in a variety of sports, such as soccer (46.5%), ice hockey (5.4%), baseball (13.6%), basketball (21%), volleyball (5.9%), and track and field events (7.6%). The sample consisted of 79 middle school students, 82 high school students, 54 university students, and 25 professional athletes.
The participation criteria were as follows: First, participants were required to enroll in a clinic-based rehabilitation program; Second, participants had to attend physical therapy sessions for at least four weeks; Third, participants must have had at least four weeks of rehabilitation remaining; Lastly, participants had to be competitive athletes.
Procedures
Item responses to the RCQ’s 95 items were measured via a five-point agree/disagree Likert scale. Expert consultations were used to test the inter validity of the RCQ test and were conducted using descriptive statistics analyses (mean, standard deviation, kurtosis, skewness, response rate). Analyses of the collected data were conducted via item analysis, including item-to-total correlations. Following the reliability analysis, an exploratory factor analysis (maximum likelihood estimation with oblique rotation) was applied to the data. A confirmatory factor analysis was applied to the measurement model to test the dimensionality of the RCQ.Convergent, discriminant validity, cross validity and predictive validity analyses were also performed to test external validity of the RCQ. All data was analyzed using Statistical Package for the Social Sciences (SPSS 18.0) and AMOS.
Study 2
Participants
The sample group comprised 52 injured athletes, between 13 to 25 years of age, who were treated and diagnosed at the Sporting Medicine Unit of Sol-hospital. These athletes were competing in international (7.7%), national (11.5%), provincial (32.7%), and regional (48.1%) events at the time of the study. The sports the athletes participated in were soccer (35.5%), ice hockey (8.3%), baseball (12.7%), basketball (16.4%), volleyball (12.7%), and track and field events (15.4%). The sample consisted of 18 middle school students, 21 high school students, eight university students, and five professional athletes. All participants had sustained moderate to severe injuries, which had kept them from attending practices and/or competitions for at least four consecutive weeks. For this study, qualifying participants must have missed a minimum of four weeks out of practice/competition due to their injuries. Injury severity was determined by using the Colorado Injury Reporting System (Blackwell & McCullagh, 1990).
Measures
Convergent Validity Measure
The Pearson correlation between RCQ subscales and the measures of theoretically related constructs were used to assess the convergent and discriminant validity of the RCQ. The Competitive State Anxiety Inventory-2 (CSAI-2; Martens, Vealey, & Burton, 1990), Profile of Mood States (POMS; McNair et al., 1971), and Rehabilitation Adherence Questionnaire (Fisher et al., 1988) were used to examine evidence for the convergent validity of the RCQ.
The CSAI-2, a multidimensional measure of competitive state anxiety, includes three scales of nine items that measures cognitive state-anxiety, somatic state-anxiety, and state-confidence on a five-point, Likert scale (0=not at all; 4=very much so).
In order to assess the injured athletes' emotions, the POMS scale was used. The POMS included scales for tension (T), depression (D), anger (A), vigor (V), fatigue (F), and confusion (C). All questionnaires used in this study were translated using a double back-translation procedure. Bivariate Pearson correlations were used to assess the hypotheses, bearing on the convergent relationship among the RAQ, CSAI-2 and POMS subscales.
RAQ was a self-report inventory with subscales designed to assess (a) perceived exertion, (b) pain tolerance, (c) self-motivation, (d) support from significant others, (e) scheduling, and (f) environmental conditions. Fisher et al. (1988) found that high scores on each of the subscales were associated with better adherence to clinic-based sport injury rehabilitation protocols.
Discriminant Validity Measure
The discriminant validity of the RCQ was assessed by computing the Pearson correlations between the RCQ subscales and the measures of theoretically unrelated constructs. The Task and Ego Orientation in Sport Questionnaire (TEOSQ; Duda & Nicholls, 1992) was used to examine evidence for the discriminant validity of the RCQ. The TEOSQ used a five-point Likert scale and contained a seven-item task orientation subscale, which assessed the extent to which an individual defined success in terms of learning, and a six-item ego orientation subscale, which assessed the extent to which success was viewed in terms of outperforming others.
Predictive Validity Measure
The participation levels of injured athletes in rehabilitation programs (initial, intermediate, final) were used to examine evidence for the predictive validity of the RCQ. Participation levels were defined as the participant’s level of compliance with the medically prescribed rehabilitation plans. To assess this variable, the researchers used a personalized record sheet, designed specifically for each participant in accordance with the rehabilitation plans recommended by the attending doctor. Athletes' intensity of effort during rehabilitation exercises, the frequency of which they followed the practitioner’s instructions and advice, and their receptivity to changes in the physical therapy program were calculated by the researcher, athletic trainers, and a doctor in three phases (initial, intermediate, and final). A Bivariate Pearson correlation was used to assess the hypotheses’ bearing on the significance of the relationship between the RCQ and participation level in rehabilitation program.
Procedures
During their first visits to the clinic following their injuries, the athletes were invited to participate in this research project. All those who agreed were asked to complete the RCQ, CSAI-2, POMS, RAQ, and TEOSQ questionnaires. During their initial visits, the attending doctor estimated the optimum recovery period for each injury. This information was used as a means of assessing the seriousness of the patients’ injuries and as a criterion for participation in the study. Subsequent psychological assessments were arranged to coincide with the check-up dates agreed upon by the doctor and the participants. In this way, every time the athletes came to the clinic for a medical check-up, they would complete the aforementioned questionnaires. This continued until the injured person was declared medically fit.
From the first visit, the injured athletes' participation levels in the rehabilitation program were also assessed. Of all the data collected, only data coincided within the initial, intermediate, and final assessments was selected for analysis. The initial assessment was carried out when the injured person visited the clinic for the first time; the intermediate assessment was carried out based on the length of the recovery period; and the final assessment was carried out on the day the injured person was declared medically fit.
Data Analysis
The results were presented in three different sections. The first section assessed the convergent relationship between the RCQ subscales and convergent validity measures through the Bivariate Pearson correlation. The second section focused on the relationship between the RCQ subscales and discriminant validity measures through the Bivariate Pearson correlation. The third section assessed the correlation between subscales of the RCQ between the participation levels of injured athletes in the rehabilitation program (initial, intermediate, final) to examine the evidence for the predictive validity of the RCQ.
Results
Study 1
Scale Development
The main goal of this research was to develop a self-administered questionnaire that had both theoretical and conceptual relevance in rehabilitation settings; this was accomplished by reviewing sports-centric, qualitative literature of psychological responses, behavior responses to the injury, and the rehabilitation process. In accordance with previous research in this area (Evans & Hardy, 1995; Gould, Udry, Bridges, & Beck, 1997a; Podlog, Heil, Schulte, 2014; Shin, 2011; Tracey, 2003; Udry, 1997; Wiese-Bjornstal, Smith, & LaMott, 1995; Wiese-Bjornstal, Smith, Shaffer, & Morrey, 1998), psychological factors, such as personal characteristics, situational variables, cognitive responses, and emotional responses, were thought to influence both rehabilitation behavior and rehabilitation outcome. Theoretically, psychological factors can affect the rehabilitation outcome of a patient both directly and indirectly, with the latter relationship mediated by rehabilitation adherence. It was necessary to assess the psychological responses to injuries and mediated variables, such as social support and personal resources, because psychological responses and mediated variables of athletes during the rehabilitation process have been found to be associated with successful recovery. In order to ensure the rehabilitation process-specificity and the content validity of the measure, a two-step procedure was followed.
First, a broad review of mainstream and rehabilitation psychology literature was conducted in order to cover the relevant domains of psychological responses, behavioral responses, and mediated variables that could affect rehabilitation outcomes. Secondly, four qualitative rehabilitation psychological studies were examined. The researcher reviewed published research pertaining specifically to rehabilitation process of athletes (Gould et al., 1997a; Gould, Udry, Bridges, & Beck, 1997b; Podlog, Heil, Schulte, 2014; Shin, 2011; Tracey, 2003). Other studies investigating factors associated with social support (Bianco, 2001; Sherman, DeVinney, & Sperling, 2004; Udry, Gould, Bridge, & Beck, 1997) and personal variables (Malec, Brown, & Moessner, 2004) were also reviewed.
The breadth of the literature review maximized the content broadness of the measure and examined participants’ emotions, mental states, behavior, social support, and personal resources. Integrated models depicting psychological responses to sport injury and rehabilitation processes, developed in rehabilitation psychology (Wiese-Bjornstal et al., 1995; Wiese-Bjornstal et al., 1998), have considered the situational factors, as well as cognitive, motivational, and affective states, as determinants of rehabilitation behaviors. Thus, constructs such as social support (Bianco, 2001; Sherman et al., 2004; Udry et al., 1997) were seen as potential determinants of psychological responses. Also, Shin (2011) examined four factors that fit with the parameters of the construct of rehabilitation capabilities of athletes: Psychological factors, behavioral factors, social support factors, and personal resource factors. Based on previous research (Bianco, 2001; Fisher et al., 1988; Shin, 2011; Gould et al, 1997a; Gould et al, 1997b; Tracey, 2003; Wiese-Bjornstal et al., 1998), a questionnaire encompassing five factors that matched the necessary parameters of the construct was developed. Using a theoretically based approach to scale development (Clark & Watson, 1995; DeVellis, 1991), six sport-relevant, homogeneous, and conceptually distinct subfactors associated the rehabilitation capability of rehabilitating athletes were identified and used to form the core of the questionnaire.
Creation of Items
95 items with five factors were developed by a quantitative assessment of literature related to rehabilitation. Experts referred to research to maximize their clarity, their specificity, and the shortness of items based on guidelines for wording items (Clark & Watson, 1995). Each item was written so that 13-year-old athletes could understand them.
The adequacy of the 95 items made through the inductive method and literature review were tested by two sports psychology professors and a psychometric professor in the first stage. In the second stage, three researchers agreed on 74 of these items, yielding an inter-judge reliability coefficient of .78. After closer examination, three researchers agreed that 9 of the 74 items overlapped significantly. After eliminating highly redundant items, this reexamination resulted in a total of 60 items. In the final stage, three researchers were asked to categorize the 60 items based on content similarities.
Assessment of Items
Participants were instructed to rate the clarity of each item and to give comments, along with alternative formulations, for items that were not totally clear. Items were also presented to one rehabilitation psychology consultant and one doctor working in the rehabilitation hospital. Using a dichotomous scale, they were instructed to assess the applicability of each item to the rehabilitation process. Based on the ratings provided by athletes, the rehabilitation psychology consultant, the doctor, and their numerous comments, some items were rewritten in order to improve their clarity and to broaden their applicability across sports type and phases of rehabilitation. Items of the RCQ are presented in table 1.

Item Information of RCQ
Procedures
The 240 athletes were contacted by researchers, who provided them with an explanation of the purposes and procedures of the research project. The athletes allowed researchers to meet them under a trainer’s supervision at the end of a training session. Athletes were asked to participate in the study during these meetings. They were told the exact purpose of the study and that the questionnaire would take 10–20 minutes to complete. A strong emphasis was put on the confidentiality of data, and athletes were instructed not to write their names on the questionnaire and to put it in an unmarked envelope before returning it to their trainers. Participants were instructed to be sincere, serious, and to complete their questionnaire individually in a quiet environment when they had enough time.
Descriptive Statistics Analysis
The means of the RCQ items ranged from 2.338 to 4.617 and their standard deviations ranged from .52 to 1.299, thus suggesting that some items could not accurately discriminate the emotions, mental states, behaviors, and social support resources of injured athletes. Consequently, 14 items (Q10, Q12, Q14, Q15, Q17, Q20, Q26, Q32, Q44, Q45, Q51, Q53, Q59, Q60) with a mean greater than 4.5 and a standard deviation of less than .10 were omitted from further analyses (Tak, 1996).
The univariate skewness values of the RCQ items ranged from -1.312 to 5.782 and their univariate kurtosis values ranged from -1.250 to 11.471, thus suggesting that some items deviated severely from normal distribution. Consequently, six items (Q3, Q8, Q18, Q30, Q43, Q46) with a skewness greater than ±3.0 and a kurtosis greater than ±8.0 were omitted from further analyses (West, Finch, & Curran, 1995). Also, two items (Q6, Q21) with a response rate greater than 50% on a scale were excluded from further analyses (Eum, 1996).
Item Analysis
Inter-item correlations were calculated for all 38 items. The goal of item analysis was to identify redundant items, because large scales often place severe limitations on clinical utility, particularly in busy medical settings. Consistent with other research and recommendations (DeVellis, 1991; Rapee, 1994), redundancy was defined in two ways: (1) A high level of inter-item correlation (r>0.45), and (2) similar content. When items met both criteria, we deleted the item with the lower item-total correlation coefficient and retained the item with the higher coefficient (DeVellis, 1991).

Descrition Analysis of RCQ
Item-total correlations were calculated for the remaining 38 items in order to produce a scale measuring a relatively specific construct and following DeVellis’ (1991) suggestion, items with the lowest corrected item-total correlations (rit≦.30) were excluded. This process was repeated until the internal consistency of the scale could not be increased further by additional item deletion (Gregory, 1996). This procedure resulted in the exclusion of nine items (Q2, Q11, Q23, Q29, Q37, Q38, Q42, Q48, Q58), reducing the total to 29 items. The corrected item-total correlations were assessed for 29 items of the RCQ, with correlations for all items being greater than 0.30 (see Table 3). As indicated, there were no more items that would have increased the scale’s reliability if they were deleted. Cronbach’s alpha for the overall scale was high (alpha=.925), as were alpha coefficients for each of the subscales (emotive factor r=.86; cognitive factor r=.81, behavioral factor r=.83, social support factor r=.78, and personal resources factor r=.80).

Item Analysis of RCQ
Exploratory Factor Analysis
Following the reliability analysis, an exploratory factor analysis (maximum likelihood estimation with oblique rotation) was applied to the data in order to investigate the factor structure of the 29-item RCQ. The resulting factors were subjected to oblique (Oblimin) rotation because we expected the subfactors of the RCQ to correlate with one another. The number of factor to retain was evaluated using (a) Kaiser’s (1961) eigenvalue >1 factor extraction rule, (b) scree plot analysis (Cattell, 1966), and (c) the interpretability of the resulting factor structures (Gorsuch, 1983).
Kaiser-Meyer-Olkin index of sampling adequacy was .83, indicating that the items were appropriate for common factor analysis using maximum likelihood estimation. Cattell’s scree plot analysis identified adequate factor number. Result of Cattell’s scree test indicated that a four-factor solution was the most interpretable. Consequently, four items (Q22, Q54, Q55, Q56) representing personal resources factor did not emerge as viable factors, as indicated by low factor loadings and/or high cross-loadings. In light of factor analysis results, the personal resources factor was discarded. In addition, one item each from emotional factor (Q28), cognitive factor (Q27), and social support factor (Q47) was deleted due to high cross-loadings or factor loadings below .50(Tak, 1996). The four factors retained were: Emotional factor (six items), cognitive factor (six items), behavioral factor (five items), and social support factor (five items). The four-factor solution of the 22-item RCQ is presented in Table 4.

Exploratory Factor Analysis
Confirmatory Factor Analysis
The fit of the three measurement models, shown in tables 5 and 6, were tested at this stage. Four-factor measurement model (22 items) exhibited a non-significant chi-square as well as a GFI, AGFI, and CFI greater than .90, and an RMSEA below .08. This result indicated that the RCQ had four factors: An emotional factor, cognitive factor, behavioral factor, and social support factor. Furthermore, the magnitudes of the factor loading estimates of four-factor measurement model (22 items) shown figure 1 ranged from .594 to .820, where a majority of the factor loadings were higher than .60. Also, internal consistency reliability estimates exceeded the .70 cut-off value recommended by Nunnally (1978).

Fit statistics of Confirmatory Factor Analysis by Model

Confirmatory Factor Analysis of RCQ
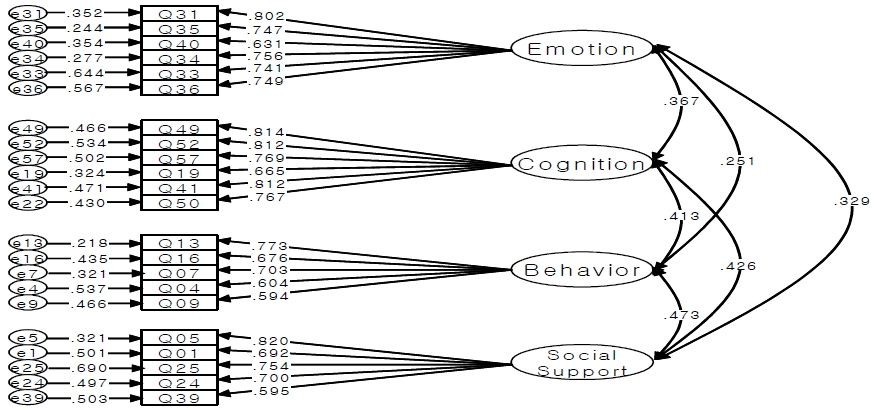
Model of Confirmatory Factor Analysis of RCQ
Study 2
Convergent Validity and Discriminant Validity
Convergent and divergent validity of the RCQ were assessed by computing the Pearson correlation between RCQ subscales and measures of theoretically related and unrelated constructs. The Pearson correlation analysis revealed moderate to high correlation between the emotion score of the RCQ and the subscale score of POMS-related emotion measurement (range, r=-.56-.79). As expected, the correlation between the emotion score of the RCQ and the POMS subscales score were high and significant; both instruments were designed to assess emotion. The Pearson correlation analysis revealed a moderate to high correlation between the cognition score of the RCQ and subscales score of CSAI-2-related cognition measurement (range, r=-.82-.78). The correlation between the cognition score of the RCQ and POMS subscales score were high and significant; both instruments were designed to assess cognition. The Pearson correlation analysis revealed a moderate to high correlation between the behavior score of the RCQ and subscales (perceived exertion, scheduling) score of the RAQ-related behavior measurement of injured athletes (range, r=.49-.55). As expected, the correlation between the behavior score of the RCQ and the subscales score of the RAQ were high and significant; both instruments were designed to assess the behavior of injured athletes. Pearson correlation analysis revealed a moderate to high correlation between social support score of the RCQ and subscales (support from significant others) score of the RAQ-related social support level of injured athletes (range, r=.81). As expected, the correlation between social support score of the RCQ and subscales score of RAQ were high and significant; both instruments were designed to assess the social support level of injured athletes.

Convergent and Divergent Validity of RCQ
Predictive Validity
In psychometrics, “predictive validity” refers to empirical evidence that demonstrates a scale has predictive power over the unobservable construct that it is intended to measure. For example, the validity of a cognitive anxiety test for performance is the correlation between cognitive anxiety scores and performance level. Correlations between subscales of the RCQ between the participation levels of injured athletes in rehabilitation programs (initial, intermediate, final) were significant, with the exception of the social support factor. There was no relationship between the social support factor and the participation level of injured athletes in rehabilitation program in the intermediate phase. The predictive validity's results are presented in table 8.

Predictive Validity of RCQ
Discussion
The purpose of this study was to develop a questionnaire that could measure the construct of rehabilitation capabilities of injured athletes. Based on the results of Study 1, it appears that the RCQ could measure rehabilitation capability, specifically as it pertains to four factors: The emotional factor, cognitive factor, behavioral factor, and social support factor. Individual resources were classified as other subfactors in the factor analysis. This result indicated that personal resource items were significant related to cognitive resources, emotional resources, behavioral resources, and social support resources.
Psychometric properties of the RCQ in this study were consistent with previous studies (Podlog, Heil, Schulte, 2014; Shin, 2011; Wiese-Bjornstal, Smith, & LaMott, 1995; Wiese-Bjornstal, Smith, Shaffer, & Morrey, 1998), which explored various subscales (emotional factor, cognitive factor, behavioral factor, and social support factor) related to rehabilitation capability. Although these findings provided preliminary evidence that the RCQ could assess rehabilitation capability, it was important for future research to confirm the factor structure and further examine the psychometric properties of the RCQ in more diverse, independent samples to determine the replicability of the observed results.
The significant inter-correlation of RCQ subscales indicated that rehabilitation capability appeared to be a multidimensional construct, with factor analysis suggesting that fit statistics of the RCQ could most parsimoniously be accounted for by a four-factor solution. Additionally, the high level of internal consistency for the entire scale indicated that computing a total score was appropriate and useful for research and/or clinical screening activities. For example, using the total RCQ score, it might be possible to easily identify injured athletes who have particularly low levels of (overall) rehabilitation capability. However, using the subscale scores, it also might be possible to identify which specific aspects of rehabilitation capability were elevated and in need of clinical intervention for particular athletes. Such information could be useful for treatment planning during the rehabilitation process.
The moderate to high correlations of the RCQ scales with the POMS, CSAI-2 (cognitive state anxiety, self-confidence), and specific subscales of the RAQ (perceived exertion, scheduling, support from significant others) indicated that the RCQ had good convergent validity properties. Also, these correlations also indicated that the RCQ measures the rehabilitation capabilities of injured athletes in a more specific way than the POMSI, CSAI-2, and RAQ, which assess the emotional, cognitive, behavioral, and social support of injured athletes.
The rehabilitation capabilities of injured athletes were not conceptually related to the TEOSQ. Consequently, the absence of significant correlations of the RCQ scales with TEOSQ supported discriminant validity of the RCQ. Significant correlation in subscales of the RCQ between the participation levels of injured athletes in rehabilitation programs (initial, intermediate, final), with the exception of the social support factor, supported the predictive validity of the RCQ. In summary, this study showed good psychometric properties of the RCQ, but further analysis is necessary to examine its test–retest reliability. Based upon our findings, future researchers will be in a good position to examine whether the RCQ is a useful screening tool for medical and psychological healthcare providers. For example, using the RCQ, athletes with low levels of rehabilitation capability could be identified and referred for cognitive-behavioral treatment to aid in their successful recovery. Following referral, the RCQ also might be useful for identifying the most pertinent treatment targets and for measuring the effectiveness of interventions targeting specific components of rehabilitation.
First, although our findings provided important support for the RCQ as an index of rehabilitation capability of injured athletes in the rehabilitation process, a number of aspects of the scale required further psychometric evaluation. Given the relative heterogeneity of our sample, future studies should indicate homogeneous samples with similar events, genders, performance levels, injury severity, and so on. Second, test–retest data for the scale is needed to establish the reliability of the scale over time. Third, future research should assess whether the RCQ can detect changes in rehabilitation capability, specifically changes that may follow a cognitive-behavioral intervention for successful recovery. Lastly, it was not easy to get a significant number of rehabilitating athletes to develop a RCQ. In this study, 240 research participants were enrolled, 120 were used for factor search, and the rest were used to verify the factor structure through confirmatory factor analysis. In the follow-up study, more research participants are needed to conduct a multi-population analysis.
References
Andersen, M. B., & Williams, J. M. (1988). A model of stress and athletic injury: Prediction and prevention. Journal of Sport and Exercise Psychology, 10, 294–306.
Andersen M. B., et al, Williams J. M.. 1988;A model of stress and athletic injury: Prediction and prevention. Journal of Sport and Exercise Psychology 10:294–306. 10.1123/jsep.10.3.294.Bianco, T. (2001). Social support and recovery from sport injury: Elite skiers share their experiences. Research Quarterly for Exercise and Sport, 72(4), 376-388.
Bianco T.. 2001;Social support and recovery from sport injury: Elite skiers share their experiences. Research Quarterly for Exercise and Sport 72(4):376–388. 10.1080/02701367.2001.10608974.Blackwell, B., & McCullagh, P. (1990). The relationship of athletic injury to life stress, competitive anxiety and coping resources. Athletic Training, 25, 23–27.
Blackwell B., et al, McCullagh P.. 1990;The relationship of athletic injury to life stress, competitive anxiety and coping resources. Athletic Training 25:23–27.Butcher, J. N., Dahlstrom, W. G., Graham, J. R., Tellegen, A., & Kaemmer, B. (1989). MMPI-2: Minnesota Multiphasic Personality Inventory-2: Manual for administration and scoring. Minneapolis: University of Minnesota Press.
Butcher J. N., Dahlstrom W. G., Graham J. R., Tellegen A., et al, Kaemmer B.. 1989. MMPI-2: Minnesota Multiphasic Personality Inventory-2: Manual for administration and scoring Minneapolis: University of Minnesota Press.Churchill, G. A. (1979). A paradigm for developing better measures of marketing constructs, Journal of Marketing Research, 16, 64–73.
Churchill G. A.. 1979;A paradigm for developing better measures of marketing constructs. Journal of Marketing Research 16:64–73. 10.2307/3150876.Clark, L. A., & Watson, D. (1995). Constructing validity: basic issues in objective scale development. Psychological Assessment, 7, 309–319.
Clark L. A., et al, Watson D.. 1995;Constructing validity: basic issues in objective scale development. Psychological Assessment 7:309–319. 10.1037//1040-3590.7.3.309.Cohen, R., Montague, P., Nathanson, L., & Swerdick, M. (1988). Psychological testing: An introduction to tests & measurement. Montain View, Califormia: Mayfield Publishing.
Cohen R., Montague P., Nathanson L., et al, Swerdick M.. 1988. Psychological testing: An introduction to tests & measurement Montain View, Califormia: Mayfield Publishing.Crossman, J., Jamieson J. (1985). Differences in perceptions of seriousness and disrupting effects of athletic injury as viewed by athletes and their trainer. Perceptual and Motor Skills, 61, 1131-1134.
Crossman J., Jamieson J.. 1985;Differences in perceptions of seriousness and disrupting effects of athletic injury as viewed by athletes and their trainer. Perceptual and Motor Skills 61:1131–1134. 10.2466/pms.1985.61.3f.1131.DeVellis, R. F. (1991). Scale development: theory and application. London: Sage.
DeVellis R. F.. 1991. Scale development: theory and application London: Sage.Duda, J. L., & Nicholls, J. G., (1992). Dimensions of achievement motivation in schoolwork and sport. Journal of Educational Psychology, 3, 290-299
. Duda J. L., et al, Nicholls J. G.. 1992;Dimensions of achievement motivation in schoolwork and sport. Journal of Educational Psychology 3:290–299.Eum, H. J. (1996). Research method of sports psychology. Korean Society of Sport Psychology.
Eum H. J.. 1996. Research method of sports psychology Korean Society of Sport Psychology.Evans, L., & Hardy, L. (1995). Sport injury and grief responses: A review. Journal of sport and Exercise Psychology, 17, 227-245.
Evans L., et al, Hardy L.. 1995;Sport injury and grief responses: A review. Journal of sport and Exercise Psychology 17:227–245. 10.1123/jsep.17.3.227.Fisher, A. C, Domm, N. A, Wuest, D. A. (1988). Adherence to sports injury rehabilitation programs. The Physician and Sports Medicine, 16: 47-51.
Fisher A. C, Domm N. A, Wuest D. A.. 1988;Adherence to sports injury rehabilitation programs. The Physician and Sports Medicine 16:47–51. 10.1080/00913847.1988.11709551.Green, S. L., & Weinberg, R. S. (2001). Relationships among athletic identity, coping skills, social support, and the psychological impact of injury in recreational participants, Journal of Applied Sport Psychology, 1, 40-59.
Green S. L., et al, Weinberg R. S.. 2001;Relationships among athletic identity, coping skills, social support, and the psychological impact of injury in recreational participants. Journal of Applied Sport Psychology 1:40–59.Gorsuch, R. (1983). Factor analysis (2nd ed.). Erlbaum, Hillside, NJ.
Gorsuch R.. 1983. Factor analysis (2nd ed.) Erlbaum. Hillside, NJ:Gould, D., Udry, E., Bridges, D., & Beck, L. (1997a). Stress sources encountered when rehabilitating from season-ending ski injuries. The Sport Psychologist, 11, 361-378.
Gould D., Udry E., Bridges D., et al, Beck L.. 1997a;Stress sources encountered when rehabilitating from season-ending ski injuries. The Sport Psychologist 11:361–378.Gould, D., Udry, E., Bridges, D., & Beck, L. (1997b). Coping with season-ending injuries. The Sport Psychologist, 11, 379–399.
Gould D., Udry E., Bridges D., et al, Beck L.. 1997b;Coping with season-ending injuries. The Sport Psychologist 11:379–399.Gregory, R.J. (1996). Psychological testing: history, principles, and applications, Allyn & Bacon, Needham Heights, MA.
Gregory R.J.. 1996. Psychological testing: history, principles, and applications Allyn & Bacon. Needham Heights, MA:Harter, S. A. (1982). The Perceived Competence Scale for Children. Child Development, 53, 87-97.
Harter S. A.. 1982;The Perceived Competence Scale for Children. Child Development 53:87–97. 10.2307/1129640.Hathaway, S. R., & McKinley, J. C. (1943). Minnesota Multiphasic Personality Inventory. Minneapolis: University of Minnesota Press.
Hathaway S. R., et al, McKinley J. C.. 1943. Minnesota Multiphasic Personality Inventory Minneapolis: University of Minnesota Press.Mainwarring, L. (1999). Restoration of self: A model for the psychological response of athletes to serve knee injuries. Canadian Journal of Rehabilitation, 12, 145-156.
Mainwarring L.. 1999;Restoration of self: A model for the psychological response of athletes to serve knee injuries. Canadian Journal of Rehabilitation 12:145–156.Malec, J, F., Brown, A, W., & Moessner, A, M. (2004). Personality factors and injury severity in the prediction of early and late traumatic brain injury outcomes. Rehabilitation Psychology, 49 (1), 55-61.
Malec J, F., Brown A, W., et al, Moessner A, M.. 2004;Personality factors and injury severity in the prediction of early and late traumatic brain injury outcomes. Rehabilitation Psychology 49(1):55–61. 10.1037/0090-5550.49.1.55.Martens, R., Vealey, R. S., & Burton, D. (1990). Competitive anxiety in sport. Champaign, IL: Human Kinetics.
Martens R., Vealey R. S., et al, Burton D.. 1990. Competitive anxiety in sport Champaign, IL: Human Kinetics.McDonald, S. A, & Hardy, C. J (1990). Affective response patterns of the injured athlete: An exploratory analysis. The Sport Psychologist, 4, 261-274.
McDonald S. A, et al, Hardy C. J. 1990;Affective response patterns of the injured athlete: An exploratory analysis. The Sport Psychologist 4:261–274. 10.1123/tsp.4.3.261.McNair, D, Lorr M., & Droppleman, L. (1971). Profile of Mood States (Manual). San Diego: EDITS.
McNair D, Lorr M., et al, Droppleman L.. 1971. Profile of Mood States (Manual) San Diego: EDITS.Podlog, L., Heil, J., &Schilte, S. (2014). Psychosocial factors in sports injury rehabilitation and return to play. Physical Medicine Rehabilitation clinics, 25 (4), 915-930.
Podlog L., Heil J., et al, Schilte S.. 2014;Psychosocial factors in sports injury rehabilitation and return to play. Physical Medicine Rehabilitation clinics 25(4):915–930. 10.1016/j.pmr.2014.06.011.Shin. J. (2011). The exploration on factors affecting rehabilitation outcome of injured athletes during rehabilitation process. Journal of Korean Society and Sports Leisure, 43, 705-718.
Shin J.. 2011;The exploration on factors affecting rehabilitation outcome of injured athletes during rehabilitation process. Journal of Korean Society and Sports Leisure 43:705–718.Shin. J., & Yook, D. (2011). The Effects of Emotional․ Cognitive Psychology factor and Rehabilitation Adherence on Recovery of Sport Injury. The Korean Journal of Physical Education, 44(3), 249-259.
Shin J., et al, Yook D.. 2011;The Effects of Emotional․ Cognitive Psychology factor and Rehabilitation Adherence on Recovery of Sport Injury. The Korean Journal of Physical Education 44(3):249–259.Tak, J. K. (1996). Method of psychology test. Seoul: Hakjisa.
Tak J. K.. 1996. Method of psychology test Seoul: Hakjisa.Tracey, J. (2003). The emotional response to the injury and rehabilitation process. Journal of Applied Sport Psychology, 15(4), 279-293.
Tracey J.. 2003;The emotional response to the injury and rehabilitation process. Journal of Applied Sport Psychology 15(4):279–293. 10.1080/714044197.Udry, E. (1997). Coping and social support among injured athletes following surgery. Journal of Sport & Exercise Psychology, 19, 71-90.
Udry E.. 1997;Coping and social support among injured athletes following surgery. Journal of Sport & Exercise Psychology 19:71–90. 10.1123/jsep.19.1.71.Udry, E., Gould, D., Bridge, L., & Beck, L. (1997). Down but not out: Athlete response to season-ending injuries. Journal of Sport & Exercise Psychology, 19, 229-248.
Udry E., Gould D., Bridge L., et al, Beck L.. 1997;Down but not out: Athlete response to season-ending injuries. Journal of Sport & Exercise Psychology 19:229–248. 10.1123/jsep.19.3.229.West, S. G., Finch, J. F., & Curran, P. J. (1995). Structural equation modeling with non-normal variables: problems and remedies. In R. H. Hoyle, Structural equation modeling (pp. 56–75). Thousand Oaks, CA: Sage.
West S. G., Finch J. F., et al, Curran P. J.. 1995. Structural equation modeling with non-normal variables: problems and remedies. In. Hoyle R. H.. Structural equation modeling p. 56–75. Thousand Oaks, CA: Sage.Wiese-Bjornstal, D. M, Smith, A. M, Shaffer, S. M, Morrey, M. A. (1998). An integrated model of response to sport injury: Psychological and sociological dynamics. Journal of Applied Sport Psychology, 10, 46-49.
Wiese-Bjornstal D. M, Smith A. M, Wiese-Bjornstal Shaffer, Morrey M. A.. 1998;An integrated model of response to sport injury: Psychological and sociological dynamics. Journal of Applied Sport Psychology 10:46–49. 10.1080/10413209808406377.Appendices

