Musculoskeletal Injury Patterns among Korean Professional Women Soccer Players: A Retrospective Descriptive Study
Article information
Abstract
Female Korean professional soccer players endure a high burden of injuries throughout their careers. This retrospective study investigated their injury history characteristics by surveying 181 players across eight Korea Women’s Football Federation teams. The survey covered demographics, playing positions, career spans, dominant legs, national team memberships, and detailed information on previous injuries, including location, type, mechanism, and severity. Analysis revealed lower extremities as the most vulnerable region, injured in 44.7% of competitions, and 46.6% of practice sessions, followed by foot and ankle injuries. Joint and ligament injuries dominated, comprising 45.0% of competition-related incidents, and 55.2% of those sustained during practice. Notably, contact was the primary mechanism for practice injuries (49.8%), while overuse (33.4%) and contact (33.2%) shared the blame in competitions. Interestingly, severe injuries were significantly more prevalent in practice (65.2%) compared to competitions (48.2%). Almost all players had at least one previous injury, often affecting the lower extremities. This highlights the need for targeted preventive measures addressing the high prevalence of severe joint and ligament injuries, often exacerbated by aggressive situations. These findings emphasize the crucial need for tailored injury prevention strategies specifically designed for the unique demands and challenges faced by women’s soccer players.
Introduction
Women’s football has grown exponentially in recent years and has become one of the most popular team sports worldwide (Fédération Internationale de Football Association [FIFA], ; Valenti et al., 2018). The FIFA reported a notable presence of more than 30 well-established national leagues dedicated to women’s football, with global participation of over 13 million women in organized football, encompassing both amateur and elite levels (FIFA, 2019). Women’s soccer is officially played in over 100 countries, with thriving leagues primarily focused on various countries across Europe and North America (FIFA, 2014, 2019). As of 2021, South Korean women’s football has more than 1,400 elite players registered across 63 teams (Korean Football Association, 2021).
Although participating in soccer has several associated health-related benefits such as postural control and cardiovascular and muscular adaptations (Jakobsen et al., 2011; Krustrup et al., 2009, 2010; Oja et al., 2015; Randers et al., 2012), the high physical demands inherent in training and games, coupled with frequent exposure to physical contact and tackles, may increase the risk for injury to female players (Faude et al., 2006; López-Valenciano et al., 2021). The risk for these injuries may be higher in professional leagues, as the professional level and popularity of women’s football have increased significantly in recent years. Among women’s sports, soccer had the highest competition injury rate (17.2 estimated injury rate per 1,000 athlete exposures), which was high when compared to men’s sports (Kerr et al., 2015). Musculoskeletal injuries may have short- and long-term negative physical, psychological, and financial consequences on individual athletes and their teams, and a history of injuries can affect physical and mental health during retirement (Eliakim et al., 2020; Kerr et al., 2014; Lee, Jeon, et al., 2020; Marchi et al., 1999).
Therefore, injury surveillance research should be conducted to collect data on the location, type, timing, cause, and mechanism of injury to provide a basis for understanding the causes and risk factors of injury and, ultimately, for prevention (Bahr & Krosshaug, 2005; Finch, 1997, 2006). Several epidemiological studies in female soccer players have shown that 51–83% of injuries occur through physical contact with other players (Junge & Dvorak, 2013; Soligard et al., 2010) and 19–39% are due to foul play (Jacobson & Tegner, 2007; Junge & Dvorak, 2013). Notably, 69–90% of female soccer injuries were classified as traumatic (sudden-onset injury, from a single incident with a known trauma) (Faude et al., 2005; Jacobson & Tegner, 2007; Le Gall et al., 2008; Soligard et al., 2010; Steffen et al., 2008; Tegnander et al., 2008), and most injuries were located in the lower extremities. Knees, ankles, and thighs were the most common locations for injury in female players (Clausen et al., 2014; Faude et al., 2005; Jacobson & Tegner, 2007; Le Gall et al., 2008), although the knee has typically been referred to as the most frequent location for severe injuries (Faude et al., 2005; Jacobson & Tegner, 2007; Le Gall et al., 2008). The most frequently diagnosed injury type was sprains and strains, with ankle sprains having the highest prevalence in both young (Le Gall et al., 2008; Söderman et al., 2001; Steffen et al., 2008) and elite female soccer players (Faude et al., 2005; Tegnander et al., 2008). A recent study analyzing the injury characteristics of women’s national soccer players in Korea reported results consistent with the previous studies. Most injuries that occurred during training and competition involved the lower extremities (79%). The most common type of injury was muscle rigidity (45.0%), followed by contusions/hematomas/bruises (22%) and sprain (15%). Minimal injury (1–3 days, 67%) was the most common injury, followed by mild (29%), moderate (3.5%), and severe (1%) injuries (Joo, 2022). However, the previous study had a few limitations, including that the injury information in Korean soccer players was investigated only during national team call-ups. Furthermore, some studies were limited by not considering the injury history of the individuals.
In the context of a dynamic model of etiology in sports injuries, the injury history of an individual assumes a crucial role as a critical risk factor (Meeuwisse et al., 2007; van Mechelen et al., 1992). Injury history is attributable to its substantial influence on the likelihood of re-injury, and also to its interaction with intrinsic and extrinsic factors for new and/or re-injury (Meeuwisse et al., 2007). Among female soccer players, the occurrence of previous injuries resulted in low subjective function in the involved region (up to 11% decrease), ultimately increasing susceptibility to subsequent injuries within the same anatomical region (rate ratio 1.2–1.6) (Steffen et al., 2008). Considering the notable incidence of injuries among youth and adolescent female soccer players, a substantial accumulation of injuries may tend to occur by the time they transition into the professional level (Söderman et al., 2001; Steffen et al., 2008). This tendency is because young players potentially returned to the field extremely early and/or without sufficient rehabilitation to alleviate the deficits/symptoms resulting from the injury in the involved segment or joint. Injuries may have a negative impact on overall health and quality of life by causing early degeneration and limiting future physical activity (Russell et al., 2018; Saltzman et al., 2005); therefore, it is important to assess the cumulative history of injuries in elite athletes who have been playing from a young age and develop an injury prevention/management strategy. Retrospective epidemiological studies are needed as the first step in maintaining and improving performance, lengthening playing careers, and improving the quality of life of retired female soccer players.
Recently, several epidemiological studies presented standardized injury profile reporting systems by investigating the etiology of injuries, such as location, type, mechanism, and severity, based on the FIFA Medical Assessment and Research Centre (F-MARC) consensus statement and the International Olympics Committee Injury Surveillance System (IOC-ISS) to suggest standard information (Engebretsen et al., 2013; Fuller et al., 2006; Junge et al., 2009; Lee, Jeong, et al., 2020; Soligard et al., 2017). However, only a few studies have examined data on injuries during the Korean Women’s Professional Soccer League. One possible explanation for the limited profile of soccer injuries is the absence of a soccer injury monitoring system for Korean women. Considering the rapid development of elite women’s football, research is needed to analyze the injury profiles of top-level players to develop appropriate prevention strategies specifically for women. Therefore, this study determined past injury status by surveying female Korean professional soccer players. Based on the need for comprehensive injury data and prevention strategies tailored to the unique demands of female soccer, the following questions are proposed: 1) Does a substantial proportion of female soccer players have a history of injuries? 2) What are the primary anatomical locations, injury types, levels of severity, mechanisms, and temporal patterns associated with injuries in female soccer players? This will help develop rehabilitation and injury prevention programs to improve the performance of female Korean soccer players. Furthermore, this study may contribute to establishing an injury surveillance system to collect retrospective injury histories and injury data during further seasons in Korean women’s soccer.
Methods
Participants
In 2020, an injury history survey was conducted among eight professional teams registered with the Korean Women’s Football Federation. Out of 200 players from eight teams, 181 players participated in the survey, excluding 11 players of foreign nationality and eight who did not agree to participate in the study due to personal reasons. The demographic characteristics of all participants are shown in Table 1. The researchers visited each team and conducted the survey between March and May 2020. This study was approved by the Institutional Review Board of Yonsei University (No. 7001988-202005-HR-887-03), and written informed consent was obtained from all players prior to their participation and from the doctors in each team.

Demographic characteristics of female korean professional soccer players
Injury Report Forms and Data Collection
The researchers instructed all participants to fill out a questionnaire regarding their injury histories. The questionnaire consisted of questions regarding demographic information such as playing position, athlete career, dominant leg, and whether to convene as members of the national team. Players were asked to provide details regarding past injuries, including type, severity, location, and injury mechanism, based on the F-MARC and IOC-ISS surveys (Fuller et al., 2006; Junge et al., 2008).
Injury was defined as any physical damage that occurred during soccer activities (scheduled matches or training sessions) that resulted in the player being unable to completely participate in the training sessions or matches. A player was considered injured until the team doctor allowed complete participation in team training and match play (Fuller et al., 2006). The physician specified whether the injury was sustained during a match or during training and whether it was induced by a contact with another player (defined as contact injury) or not (defined as non-contact injury). Injury severity was graded according to the number of absences from complete soccer activities such as team training or a match after injury diagnosed by medical doctors: (1) “slight” injury indicating 0 days lost, (2) “minimal” injury indicating 1–3 days lost, (3) “mild” injury indicating 4–7 days lost, (4) “moderate” injury indicating 8–28 days lost, and (5) “severe” injury indicating >28 days lost (Fuller et al., 2006). Soccer injuries were classified using an adapted version of the Orchard Sports Injury Classification (Rae & Orchard, 2007). The questionnaire included specific items to identify the location on the body (including side) and the type of injury.
Statistical Analysis
The retrospective injury information obtained from the questionnaires were described as absolute and relative frequencies with categorical variables. Chi-square test was performed to establish the significance of the difference between female soccer players who suffered injuries during competition and those who suffered injuries during practice by any specific injury location, type, mechanism, or severity. All data were analyzed using the IBM SPSS software (version 25.0; IBM Corp., Armonk, NY, USA). The alpha level for all analyses was set at .05.
Results
A total of 650 injuries were reported in 181 female soccer players. The location, type, mechanism, and severity of the retrospectively investigated injuries are shown in Tables 2–4, and Table 5 shows the different injury characteristics between the games and practice. All injury data is summarized in Figure 1.
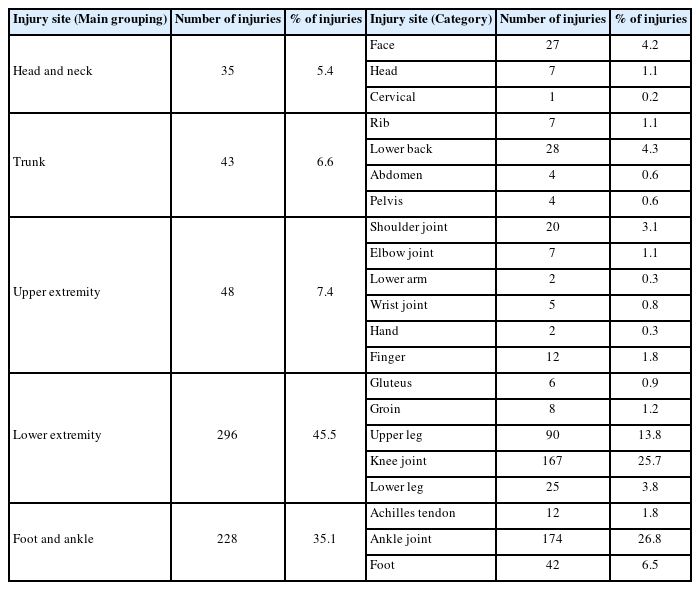
Injury location in past injury characteristics
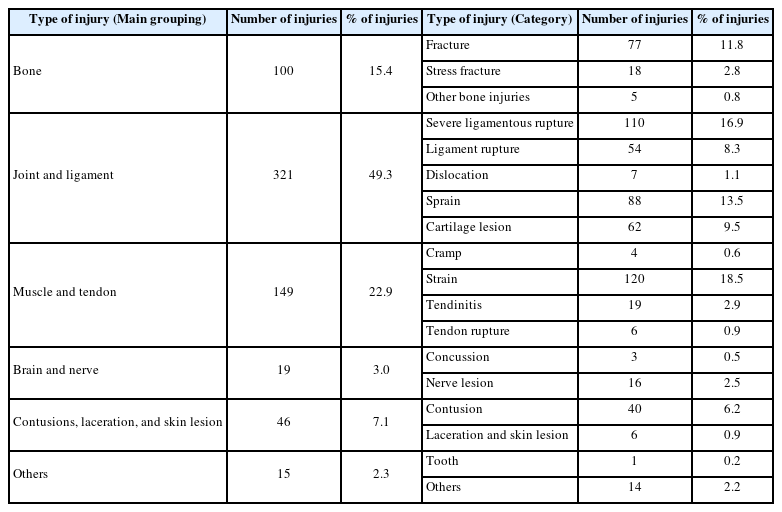
Injury type in past injury characteristics
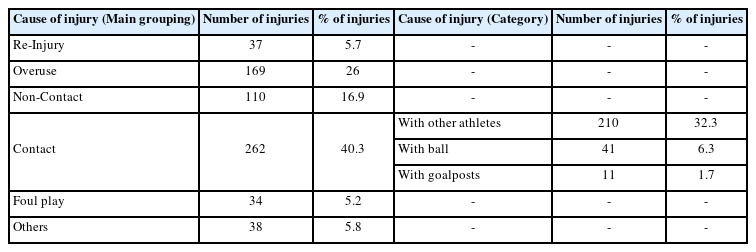
Injury mechanism in past injury characteristics
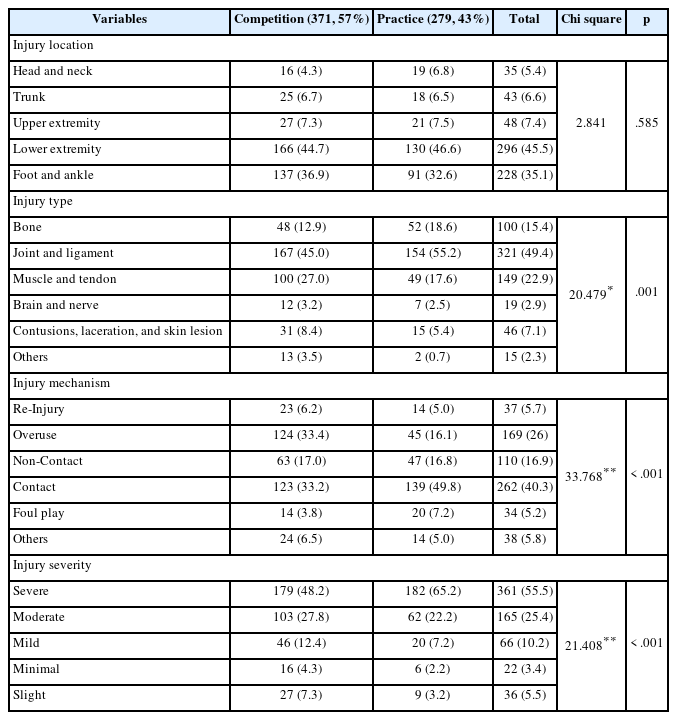
Past injury characteristics in relation to competition and practice
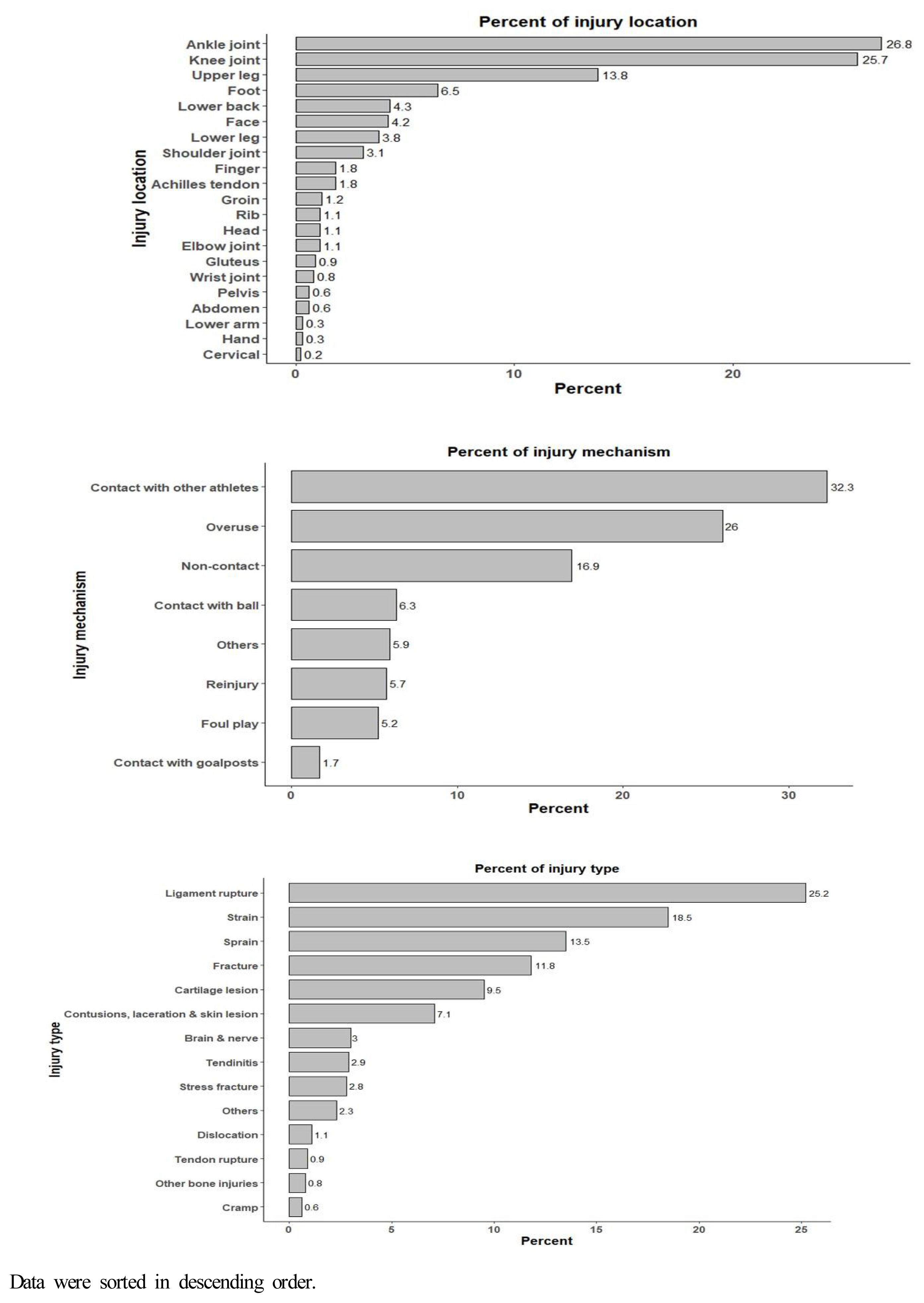
Overall summary of past injury outcomes for female soccer players.
Injury Location
Injuries were most common in the lower extremities (45.5%; n = 296). Foot and ankle injuries, classified separately into the lower extremities, were the second most common (35.1%, n = 228; Table 2). The most common injury location was the ankle joint (26.8%, n = 174), followed by the knee joint (25.7%, n = 167), upper leg (13.8%, n = 90), and foot (6.5%, n = 42). This was followed by the lower back (4.3%, n = 28), face (4.2%, n = 27), and shoulder joints (3.1%, n = 20; Table 2).
The chi-square test suggested that the proportion of injury locations (head and neck, trunk, upper extremity, lower extremity, foot, and ankle) did not vary between competition and practice (χ2 = 2.841, p = .585; Table 5). The pattern of injury occurrence was the same, with lower extremity, foot, and ankle injuries being the most common.
Injury Type
The most common types of injury were joint and ligament injuries (49.3%, n = 321), followed by muscle and tendon injuries (22.9%, n = 149), and bone injuries (15.4%, n = 100; Table 3). The most common type was strain (18.5%, n = 120), followed by severe ligamentous rupture (16.9%, n = 110), sprain (13.5%, n = 88), fracture (11.8%, n = 77), and cartilage lesion (9.5%, n = 62; Table 3).
The type of injury differed significantly depending on the game or practice (χ2 = 20.479, p = .001; Table 5). Joints and ligaments were the most frequent injury sites in competition and practice. The second most common were muscle and tendon injuries in competitions, while bone injuries were more common in practice.
Injury Mechanism
As shown in Table 4, the primary mechanism of injury observed was contact (40.3%, n = 262), with injuries resulting from contact with other players being the most prevalent (32.3%, n = 210; Table 4). Overuse (26.0%, n = 169) and non-contact (16.9%, n = 110) injuries also accounted for a large proportion of the overall injuries (Table 4).
Contact injuries were common in both competition (33.2%, n = 123) and practice (49.8%, n = 139); however, the difference in proportions suggested a difference in injury mechanisms based on the context of play (χ2 = 33.768, p < .001; Table 5). Overuse injuries (33.4%, n = 124) that occurred during competition were the most common, with overuse mechanisms being more common than those caused by contact. This was followed by injuries caused by contact and non-contact. During practice, contact injuries were the most frequent (49.8%), followed by overuse injuries (16.1%, n = 45) and non-contact injuries (16.8%, n = 47), which showed similar rates.
Injury Severity
The severity of injuries is shown in Table 5. Severe injuries (55.5%, n = 361) were most common, followed by moderate (25.4%, n = 165), mild (10.2%, n = 66), slight (5.5%, n = 36), and minimal (3.4%, n = 22) injuries.
The severity of the injury differed significantly according to the circumstances (χ2 = 21.408, p < .001; Table 5). Specifically, the pattern was the same for injuries in both competition and training, with a higher proportion of injuries progressing from mild to severe; however, there were differences in the proportion by severity.
Discussion
This retrospective epidemiological study determined the profile of injury histories among female Korean professional soccer players. Based on the injury data collected from players in the female Korean professional soccer league, the major findings were as follows: 1) The most frequently injured location during competitions was the lower extremity (44.7%), followed by the foot and ankle (36.9%). In addition, injuries that occurred during training showed the same pattern as that during competition at 46.6% and 32.6%, respectively. 2) Joint and ligament injuries were the most common during competitions (45.0%) and practice (55.2%). 3) Contact (49.8%) was the primary mechanism of injury during practice, whereas overuse (33.4%) and contact (33.2%) were the major causes during competition. 4) Injuries by female players during competitions (48.2%) and practice (65.2%) were severe.
Our retrospective results showed that the injury location in female soccer players was most common in the lower extremities and foot and ankle, and injuries in these two regions accounted for approximately 80% of the total injuries. These findings could be attributed to the manner of ball manipulation by soccer players, specifically through the utilization of their lower extremities (Joo, 2022). In addition, the imposition of a substantial load on the lower extremities as a result of high-intensity movements, such as jumping, deceleration, and abrupt changes in direction, may have substantially contributed to the heightened incidence of injuries in lower extremity (Joo, 2022). Similar to our results, previous authors found that soccer injuries occurred commonly in the lower extremities, such as ankles, knees, and upper leg region (Clausen et al., 2014; Faude et al., 2005; Jacobson & Tegner, 2007; Joo, 2022; Junge & Dvorak, 2013; Khodaee et al., 2017; Le Gall et al., 2008; López-Valenciano et al., 2021; Söderman et al., 2001; Steffen et al., 2008; Tegnander et al., 2008). Tegnander et al. (2008) prospectively observed female elite soccer players and reported that the majority of the injuries occurred in the lower extremities (81%). A study analyzing the previous injuries of female Korean national soccer players reported that lower extremity injuries were 78% and 79% of all injuries during practice and competition, respectively (Joo, 2022).
An interesting finding from our injury survey was that a large proportion of injuries were concentrated in specific joints and segments, most frequently in the ankle (26.8%), knee (25.7%), and upper leg (13.8%). Due to the lack of specific information and the limitations of the study design, a sub-analysis to identify the most prevalent specific injuries was not possible. However, these results may be supported by the findings of previous studies showing that the most common types of overuse injuries are pain in the lower leg and knee, and ankle sprains are the most common acute injury type (Steffen et al., 2008). Considering that ankle sprains are the predominant injury type in soccer regardless of sex or play level, it is unsurprising that the highest frequency of injuries was observed in the ankle region (Gaulrapp, Becker, Walther, & Hess, 2010; López-Valenciano et al., 2021; Söderman et al., 2001). Because lower extremity injuries account for most of the total injuries in female soccer players, F-MARC developed and proposed injury prevention programs such as “FIFA 11” and “FIFA 11 Plus,” which focus on improving lower extremity functions and neuromuscular control, as previous studies have confirmed (Robles-Palazón et al., 2016; Silvers-Granelli et al., 2015). In this study, considering that most injuries occurred in the ankle joint among lower extremity injuries, it is necessary to expand and apply the ankle injury mechanism and risk factors to the existing injury prevention program. Future research should identify the exact diagnosis of injuries occurring in the ankle, knee, and upper leg to refine injury prevention strategies.
In our study, the proportion of head and neck injuries needs to be highlighted (5.4%). Notably, injuries in these regions, which were the most threatening of all injuries, were more common in practice (6.8%) than in competition (4.3%). The prevalence of head and neck injuries, mainly concussions and mild traumatic brain injuries, is a matter of concern because of their potential to cause both immediate and long-term structural and functional alterations in the brain or nerve pathways. Furthermore, head and neck injury figures are likely to be even higher, as they are frequently underdiagnosed owing to reduced symptom perception and are often under-reported to medical staff (Mooney et al., 2020). Although head and neck were the least common locations of injury in our survey, a meta-analysis that prospectively examined injuries in female soccer players from Western and American countries found that head and neck injuries were the third most common after lower extremity and trunk injuries (López-Valenciano et al., 2021). In addition, head and neck injuries tend to increase by up to 21% at large sporting events such as the FIFA world cup, where competition and contact intensify (Junge & Dvorak, 2013). Athletic trainers and medical staff off-field should carefully assess injured players and conservatively move them from the field in case of strong contact to the head and neck region. Athletes should also be educated about the symptoms of concussions and head injuries to prevent themselves from being sidelined with a major traumatic injury and their sequela. Most importantly, the rate of head and neck injuries has been reduced. Strict rules against hitting other players’ heads, intentionally or unintentionally, during contests on the ground or in the air, are strategies that could be considered.
The results of this study indicated that joint and ligament injuries accounted for nearly half of all the injuries (49.4%). Joint and ligament injuries were the most common in both competition (45.0%) and practice (55.2%), but the second most common were muscle and tendon injuries in competition (27.0%) and bone injuries in training (18.6%). According to previous literature, joint injuries ranging from simple sprains to ligament tears and/or rupture exhibit the highest incidence rates, with a significantly higher prevalence observed during competitions than that during practice sessions (Gaulrapp et al., 2010; Söderman et al., 2001; Steffen et al., 2008). Along with the aforementioned findings of the most frequent injuries in the ankle and knee regions, the high incidence of injuries such as ankle sprains, meniscus lesions, anterior cruciate ligament tears, and medial collateral ligament sprain, the most common injuries in women’s soccer, can be explained (Gaulrapp et al., 2010). Furthermore, sex differences in neuromuscular activation patterns and anatomy may contribute to an increase in certain injuries, such as anterior cruciate ligament tears (Ireland, 2002); therefore, injury reduction/prevention interventions should be tailored to female football players. Balance and/or coordination training, including jumping, change of direction (agility), landing tasks, and the utilization of external support measures, such as bracing or taping, can effectively reduce the incidence of joint and sprain injuries in football players (Gulbrandsen et al., 2019; Hrysomallis, 2007; Junge & Dvorak, 2004).
We found that the majority of injuries in female football players were caused by contact with other players, the ball, and goalposts (40.3%). Notably, 32.3% of the injuries were caused by contact with another player, whereas ball (6.3%) and goalpost (1.7%) contact injuries were rare. The rapid development of women’s soccer and the exceptional physical performance of players may contribute to the high proportion of injury mechanisms related to contact with other players and foul play. Contact, including tackling, is the main mechanism for lateral ankle ligament injuries that are most common in women’s soccer, along with running and landing movements (Andersen, Floerenes, Arnason, & Bahr, 2004). The injury mechanism demonstrated through the present study and previous evidence is supported by the fact that half of the injuries during competition (48.2%) and practice (65.2%) were of severe grade. Our results are consistent with previous studies which reported that 34.3% of all injuries were due to contact consisting of “tackling” or “tackled” (Gaulrapp et al., 2010). In addition, Faude et al. (2005) reported that the majority of contact injuries occurred as a result of tackling situations, with a small number of injuries resulting from foul play and collisions (Faude et al., 2005). The aggressive play between players was probably reflected in the high rate of contact injuries in competition or practice. Therefore, strict references to unnecessary contact and foul play can significantly contribute to reducing contact injuries (Junge & Dvorak, 2013).
Non-contact injuries, which are injury mechanisms that occur without contact with other players, such as step movement, direction change, acceleration/ deceleration, and landing, were also common in our survey (16.9%). Non-contact injuries differ significantly from contact injuries in that they can be prevented by improving an individual’s neuromuscular control or by preventing movement/biomechanics aligned with the mechanism of injury occurrence by neuromuscular training (Alentorn-Geli et al., 2009). In other words, non-contact injury mechanisms are influenced by modifiable risk factors. Therefore, incorporating elements of neuromuscular control, strength, plyometric, and balance training into an injury prevention program, either during pre-training warm-up or post-training cool-down sessions, can modify sports techniques and improve conditioning.
Soccer is a contact sport that requires a high level of physical performance and specific skills. Sprints, physical competition with other players, jumps, and kicks, which require explosive muscle strength, are important movements in soccer that increase the risk for injuries. Considering that injury prevention is the key to maintaining athletic performance and living a healthy life, documenting information about the site, type, mechanism of occurrence, and severity of injury should be the first step.
This study had some limitations. First, the results may have been affected by recall bias because injury information was retrospectively collected. Second, it was not possible to report the incidence of injury because of the lack of accurate data on athletes’ exposure to practice and competition. Third, it was not possible to report more detailed information about the injuries from a medical perspective because simple epidemiological investigations were used. Despite these limitations, as this is a full survey of Korean women’s professional soccer players, it is expected that these results will be used for the development of evidence-based injury prevention programs and education to reduce the injury rate of Korean women’s soccer players.
Conclusion
In this study, conducted on professional female soccer players, nearly all participants reported having experienced at least one previous injury during their sports careers. Players suffered from a high number of lower extremity, foot, and ankle injuries. Most injuries were caused by contact mechanisms and can be prevented by improving rules and strict refereeing. The results of this study highlight the need for future prospective studies to identify the internal and external factors that lead to injury and determine the effectiveness of injury prevention interventions.
Acknowledgments
This study was conducted in cooperation with the Korean Women’s Professional Soccer League. The authors deeply appreciate the cooperation of all players and team physicians. We also thank the Institute of Convergence Science (ICONS) of Yonsei University and the International Olympic Committee (IOC) Research Centre Korea for Prevention of Injury and Protection Athlete Health.
Notes
Author Contributions
Conceptualization: L.J.M & H.G.J & S.H.I & S.Y.L
Data curation: L.J.M & H.G.J & S.H.I & S.Y.L
Formal analysis: L.J.M & H.G.J
Investigation: L.J.M & S.H.I
Project administration: S.H.I & S.Y.L
Writing—original draft preparation: L.J.M & H.G.J
Writing—review and editing: S.H.I & S.Y.L
Conflict of Interest
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors. This study did not require ethical approval because it was a secondary data analysis. The authors report there are no competing interests to declare.