The Role of Parental Physical Activity Behaviors on Parental Physical Activity Support in Parents of Children with Developmental Disabilities
Article information
Abstract
The role of parental physical activity (PA) behaviors in promoting PA support for children with developmental disabilities (DDs) is unclear. The study examined differences in parental PA support between inactive and active parents of children with DDs, and investigated the association between parental PA behaviors and three types of support: encouragement, co-participation in PA activities (co-PA), and logistical support. A total of 319 parents of children with DDs participated in an online survey. Utilizing exploratory factor analysis, independent t-tests, and multiple regression analyses, the study revealed significantly lower levels of all three types of parental PA support provided by inactive parents compared to active parents. Additionally, the dummy coded variable representing parental PA behavior groups (active vs. inactive group) emerged as a significant predictor of all three types of support: encouragement (β = −.20, p <.001), co-PA (β = −.43, p <.001), and logistic support (β = −.35, p <.001). For professionals working with families in this context, the crucial role of parental PA behaviors in shaping PA support for children with DDs should be considered.
Introduction
A large number of studies have reported physical inactivity behaviors in children with developmental disabilities (DDs) (Cacioppo et al., 2021; Case et al., 2020; Cook et al., 2015). One study using a nationally representative sample (n = 45,897) found that children with learning disabilities were 33% less likely to meet PA guidelines (i.e., 60 minutes of moderate-to-vigorous PA per week) compared to their counterparts without disabilities. Another national representative study using the National Survey of Children’s Health data set (United States) found that only 19% of children with DDs (n = 3,010) participated in 60 minutes of PA per day (Case et al., 2020). More recently, another study indicated that about 44% of children with disabilities (n = 1,000) stopped participating in PA during the COVID-19 pandemic (Cacioppo et al., 2021). Given the benefits that children can receive from PA participation, the inactivity among children with disabilities may be a serious public health concern (Centers for Disease Control and Prevention; CDC, 2020a, 2020b). In addition, a review of global data regarding the prevalence of PA indicated that individuals with disabilities are about 16% to 62% less likely to meet the WHO 2010 PA guidelines (i.e., 150 minutes of moderate-to-vigorous PA per week) (Martin Ginis et al., 2021). This result suggests that physical inactivity problems in children with DDs do not naturally resolve as they age.
One of the influencing factors for PA at the family level in children with DDs is parental PA support (Li et al., 2016). A systematic review investigated multi-level factors for PA in children with DDs based on socio-ecological theory and found that parents play an important role in promoting PA in their children (Li et al., 2016). Specifically, in the review, parental PA support was a consistent intrapersonal predictor for PA in children with DDs. Another review study provided similar results indicating that parental PA supports may be the most influential factor among parent-related factors such as parental perception and parental PA behaviors (Ku & Rhodes, 2020). A recent study found that parental PA support may be a better predictor for PA behaviors in children with DDs compared to parental PA modeling (James et al., 2022).
Given its importance, a number of studies have examined factors related to parental PA support (Brown et al., 2020; Jeong et al., 2015; Ku et al., 2020, 2022). Some studies (Brown et al., 2020; Jeong et al., 2015) have used a theory (i.e., Theory of Planned Behavior), whereas another body of literature (Ku et al., 2020, 2022) have used a conceptual model to explain parental PA support in parents of children with disabilities. Among a variety of influencing factors, parental PA behaviors have been revealed as a consistent and a reliable factor for parental PA support (Ku et al., 2020, 2022; Siebert et al., 2016). Siebert and colleagues (2016) may be the first study reporting the significant association between PA behaviors and parental PA support in parents of children with disabilities. A subsequent study was conducted by Ku and colleagues (2020), and they found that parental PA behaviors were significantly and positively associated with parental PA support in children with developmental disabilities (Ku et al., 2020). More recently, another study echoed these results, reporting a significant association between the variables (Ku et al., 2022). Even though the previous studies provide fundamental information regarding the factors associated with parental PA support, the understanding of association between parental PA behaviors and support is still limited. In particular, the association between parental PA behaviors and different types of parental PA support has not been widely studied.
Even though parental PA support is a multi-dimensional construct including sub-types of support such as encouragement, co-PA, and logistic support (Ku et al., 2022; Rhodes et al., 2020), previous studies have measured parental PA support as a unidimensional construct. Thus, the association between parental PA behaviors and the different types of parental PA support is not clear. Moreover, the differences in types of parental PA support between active and inactive parents of children with DDs have not been widely studied. It is likely that inactive parents of children with disabilities provide their children with less PA support compared to active parents of children with DDs (Ku et al., 2022). Previous studies have indicated that parents of children with DDs show inactive PA behaviors (Ku & Haegele, 2022; Ku & Sung, 2021; Lee et al., 2017). A systematic review including 12 studies found that 50% of the studies reported that parents of children with DDs do not meet the PA guidelines or participate in less PA compared to parents of children without disabilities (Ku & Sung, 2021). In addition, another study using the 2018 National Health Interview Survey found that about 52% of parents of children with DDs do not meet the PA guidelines (Ghim & Ku, 2022). Thus, it is necessary to investigate parental PA support behaviors in inactive parents of children with DDs.Therefore, the purposes of the current study were twofold: 1) examining the association between parental PA support and parental PA behaviors, and 2) examining the differences in parental PA support between inactive and active parents of children with DDs.
Methods
Participants
To be eligible for participation in the current study, participants must be at least 18 years old and have a child between the ages of 5 and 10 years and 11 months who has been diagnosed with a developmental disability. CDC guidelines were used to identify developmental disabilities, which include but are not limited to attention-deficit hyperactivity disorder, autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, learning disabilities, and other developmental delays (CDC, 2021).
Recruitment for the study was carried out through multiple channels, including an online research flyer posted on the laboratory Facebook page of one of the authors, (B.M.K). Additionally, participants were recruited through an online survey development software company, Centiment. Details regarding their recruitment process can be found on the company’s website: https://www.centiment.co/audience-panel. The current study obtained ethics approval from the institutional review board of the first author’s previous institution (Vanguard University of Southern California).
Methodology
The current study used an online survey including demographic questions, international PA questionnaire – short form, and parental PA support questionnaire for parents of children with DDs. The first page of the survey asked a question asking the participant’s chronological age and their child’s disability type. If the participant’s answer did not meet the eligibility criteria, they were automatically out of the survey. The estimated completion rate of the survey was 72% and the estimated time to complete was 10 minutes.
Demographic Questionnaire
Demographic information was gathered, including child’s and parent’s age, parent’s relationship to child (mother/father/other caregiver), ethnicity, educational attainment (ranging from no formal schooling to advanced degrees including master’s and PhDs), household income (from less than $20,000 to $100,000 or more), and the type of developmental disability the child had. If the child’s disability type was not listed, respondents were asked to provide it. Participants were given the option to select “prefer not to answer” for all demographic questions except for age and the child’s disability type.
Parental PA Support
To measure different constructs of parental PA support, the parental PA support questionnaire for parents of children with disabilities (PPSQ for PCD; Ku et al., 2022) was used in the current study. The questionnaire consists of 12 questions measuring three sub-constructs of parental PA support, including encouragement, co-PA, and logistic support (four questions for each construct). Definitions of each construct were as follows: a) Encouragement refers to the provision of verbal or nonverbal prompts that motivate the child to engage in the behavior of interest. This can include validation and affirmation of the child’s involvement or performance in the behavior. b) Co-participation in PA involves the parent directly participating in or being in close proximity to the child during the activity. c) Logistic support includes parents making provisions for their child to engage in physical activity, such as enrolling them in sports, providing transportation to places where they can participate in physical activity, or providing them with PA-related equipment to facilitate their participation. The PPSQ for PCD begins with the question, “During a typical week, how often do you provide the following types of support for your child’s physical activity or sports?” It has a six-point Likert-type scale: never, less than once a week, 1–2 times per week, 3–4 times per week, 5–6 times per week, and daily. Thus, it measures the frequency with which parents provide their child with parental PA support in a typical week. It has excellent construct-related validity evidence (x2 = 78.42 [df = 51, p = .008], CFI = 0.98, GFI = 0.94. RMSEA = 0.05). In a previous study, the internal consistencies of each construct were α = .76 (encouragement), α = .92 (co-PA), and α = .83 (logistic support) (Ku et al., 2022). In the current study, α = .80 (encouragement), α = .91 (co-PA), and α = .82 (logistic support).
Parental PA Behaviors
The PA behaviors of the participants were assessed using the International Physical Activity Questionnaire short (IPAQ-S) form, a self-reported questionnaire that has demonstrated acceptable validity and reliability for measuring physical activity behaviors in adults (Craig et al., 2003). This questionnaire has also frequently been used in studies measuring physical activity behaviors in parents of children with disabilities (Haegele et al., 2017; Ku & Haegele, 2022). In the absence of objective measures such as accelerometers and pedometers, the IPAQ-S form is recommended for assessing parental PA behaviors in parents of children with disabilities because the minutes spent in PA can be converted into weighted metabolic equivalent-minutes (Ku & Sung, 2021).
The IPAQ-S form assesses three intensity levels of physical activity: vigorous, moderate, and walking. Frequency (days per week) and duration (minutes per day) of each of these activities are measured using two different questions. Total minutes of PA at each intensity level are calculated by multiplying the frequency and duration of PA behaviors independently. As moderate-to-vigorous physical activity (MVPA) is emphasized in current PA guidelines (CDC, 2020b), the current study measured only moderate- and vigorous-intensity activities in parents of children with DDs. This approach has been used in previous studies (Haegele et al., 2017; Ku & Haegele, 2022). Total minutes of MVPA were calculated by summing the minutes spent in both moderate and vigorous intensity activities, and weekly MVPA was calculated accordingly. The current study used the weekly PA guidelines of 150 minutes of moderate-to-vigorous-intensity PA for American adults (Piercy et al., 2018) as a cut-off to determine whether parents of children with DDs met the guidelines. If parents did not meet the guidelines, they were dummy-coded as inactive parents, while they were dummy-coded as active parents.
Statistical Analysis
Descriptive analyses, including measures of central tendency (mean), variability (standard deviation), frequency, and percentage, were used to analyze demographic information and study variables, such as parental PA behaviors and the three constructs of parental PA support. Pearson correlation was utilized to examine the associations between demographic variables, parental PA behaviors, and the three constructs of parental PA support. To test the construct validity of parental PA support variables, exploratory factor analysis was conducted. The independent t-test was used to compare different constructs of parental PA support between active and inactive parents of children with disabilities.
To investigate the association between parental PA behaviors and the three constructs of parental PA support, three separate multiple regression models were run with covariates including parental chronological age, parental education, relationship to child, and household income. The dependent variables in each model were parental encouragement, co-PA, and logistic support, respectively, while the independent variables were parental PA behaviors. To determine the internal consistencies of each construct of parental PA support, the equation of Cronbach’s alpha coefficient was used (Bland & Altman, 1997). The alpha level was set at 0.05 for all regressions. All analyses were conducted using SPSS 27 and AMOS 27 (IBM, SPSS; IBM Corp., Armonk, NY).
Results
Demographic Information
The average age of parents of children with DD was 37.84 years (7.85), with a range from 20 to 71 years. Among 319 participants, 69% were mothers and 28% were fathers. Most of the participants were White or Caucasian (81.5%). Over half of all participants had at least a college degree (61.8%), and their household income ranged from less than $20,000 to $100,000 or more. Child’s average age was 8.33 years (1.92) and their age range was from 5 to 12 years. More than half the children’s disability type was learning disability (55.5%). Table 1 includes more details of demographic information of participants.

Demographic information of participants (n = 319)
Independent T-Test
Encouragement (M = 4.86, SD = .91), co-PA (M = 3.70, SD = .12), and logistic support (M = 3.53, SD = .11) were significantly lower in inactive parents of children with disabilities compared to encouragement (M = 5.20, SD = .80), co-PA (M = 4.78, SD = .94), and logistic support (M = 4.47, SD = 1.03) in active parents of children with disabilities (t = −3.21, df = 317; t = −.8.35, df = 317; t = −6.98, df = 317, respectively). All results of the independent t-test can be found in Table 2.
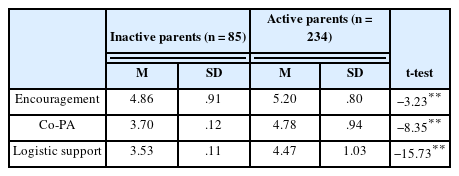
Three types of parental PA support between inactive and active parents (n = 319)
Exploratory Factor Analysis
Conducting an exploratory factor analysis revealed that a three-factor solution accounted for 61.27% of the variance, with Eigenvalues of 6.11, 1.33, and 1.04 for encouragement, co-PA, and logistic support, respectively. Four items were loaded on each construct. Due to the small sample size of the current study, a factor loading cutoff of .40 was used to determine the “goodness” of the items (MacCallum et al., 1999). With this cutoff, all loaded items were considered “good.” Except for one item (logistic support 4), factor loading values were above .5 in each construct. A detailed breakdown of the specific loadings of all items on each construct is provided in Table 3.

Factor loadings of encouragement (factor 1), co-physical activity (factor 2), logistic support (factor 3) in explanatory factor analysis (n = 319)
Correlation Matrix
The Pearson correlation revealed that parental PA behavior (dummy coding; ref: active parents) was significantly and negatively associated with three constructs of parental PA support: encouragement (r = −.17, p < .001), co-PA (r = −.42, p < .001), logistic support (r = −.36, p < .001). Encouragement was significantly and positively associated with co-PA (r = .62, p < .001) and logistic support (r = .50, p < .001). There was also a significant and positive association between co-PA and logistic support. The household income was significantly and negatively associated with encouragement (r = −.14, p = .01) and MVPAD (r = −.12, p = .02). However, it was significantly and positively associated with parental age (r = .17, p = .002) and education (r = .50, p < .001). Table 4 includes all correlation matrices of study variables included in the main analysis.
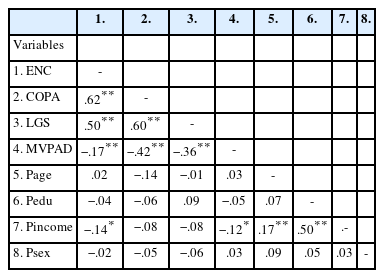
Correlation for variables included in the main analysis (n = 319)
Multiple Regression Analyses
The results of the multiple regression analyses indicate that the MVPAD variable, along with four covariates, significantly predicted parental PA support in parents of children with disabilities. Specifically, in the regression model with encouragement as the dependent variable, about 5% of the variance in encouragement was explained by the MVPAD variable with covariates including parental age, education, sex, and household income (R2 = .06, F(5,310) = 4.39, p < .001). Notably, the MVPAD emerged as a significant predictor of encouragement (β = −.20[ref: active parents], p < .001). In the multiple regression model for co-PA, about 19% of the variance in co-PA was explained by the MVPAD variable and the covariates (R2 = .19, F(5,310) = 16.56, p < .001). The MVPAD variable and parental age were significant predictors of co-PA (β = −.43[ref: active parents], p <.001, β = −.10, p =.04, respectively). Finally, in the multiple regression model for logistic support, about 12% of the variance in logistic support was explained by the parental orientation variables and four covariates (R2 =.12, F(5,301) = 9.89, P< .001). The MVPAD variable emerged as a significant predictor of logistic support (β = −.35[ref: active parents], p <.001). Additional details on the results of the three multiple regression analyses can be found in Table 5.
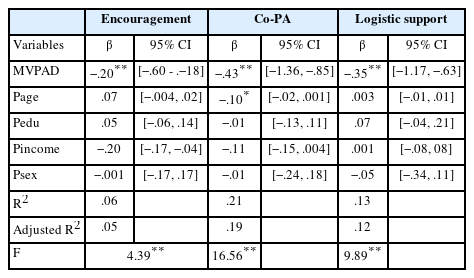
The association between the three types of parental physical activity support and parent’s physical activity behaviors (n = 319)
Discussion
Although previous studies have highlighted the role of a parent’s PA behavior in the process of parental PA support, the differences in support between active parents of children with disabilities and inactive parents of children with disabilities were not clear. Thus, one purpose of the current study was to identify the differences. In the current study, parents of children with DDs were classified into two groups based on meeting the PA guidelines (active vs. inactive). Inactive parents of children with DDs provided less of all three types of parental PA support compared to active parents of children with DDs. Specifically, co-PA in inactive parents was approximately one day less frequent (per week) compared to active parents. This finding is aligned with a previous study indicating a positive association between parental PA behaviors and co-PA (Ku et al., 2022). In particular, in that study, parental PA behaviors were a significant predictor for co-PA in the dyad of parent-child with disability even when controlling for parental orientation variables including enjoyment and importance of PA (Ku et al., 2022). This makes sense because active parents of children with disabilities may include their child in their PA time (Matos et al., 2021). For example, an active mother can intentionally walk around her community or do home exercise with her child with Down syndrome to increase her child’s PA. However, inactive parents may not be interested in doing co-PA with their child because they may have low perceived behavioral control, which is a consistent predictor for family PA (Rhodes et al., 2021). As co-PA is a strong factor that directly facilitates PA in children with disabilities (Ku et al., 2021), professionals and interventionists need to consider strategies to promote PA in the parent-disabled child dyad. Recent studies focusing on promoting PA in parents and children together (Grant et al., 2020; Ha et al., 2019) may be valuable resources to develop such strategies.
In the current study, a multiple regression model for co-PA revealed that the dummy-coded variable of parental PA behaviors was a significant predictor for co-PA. Importantly, in the model, parental age, a covariate, was significantly and negatively associated with co-PA. Even though more research should be done, a possible explanation is that older children with disabilities are likely to participate in PA with their peers, not with their parents. As children age, the type of PA can be changed from unstructured activities (e.g., running and catching balls) to structured sports (e.g., soccer and basketball) (Goodway et al., 2019). For example, it may be interesting for children with disabilities to participate in a team sports with their peer, which provides more dynamic environment and requires skill varieties. A systematic review study found a negative association between child’s age and parental PA support (Rhodes et al., 2020). Specifically, in the review study, the pooled correlation between the variables from nine independent studies was −.15 (Rhodes et al., 2020). The author of the study indicated that parents may reduce their support as their child ages, in order to promote their child’s autonomy. Instead of doing PA together, parents may provide a different type of support, such as logistic support, when their child ages because there may be more PA opportunities for older children with disabilities. A longitudinal study is necessary to untangle the association between parental age and different types of PA support.
The current study also found that logistic support in inactive parents of children with disabilities was about one day lower compared to active parents of children with disabilities. In the multiple regression model for logistic support, the dummy-coded variable of parental PA behaviors was a significant predictor for logistic support. This is an interesting finding because parents of children with DDs do not have to be physically active to provide logistic support, such as enrolling their child in sports and providing them with transportation to places where children can participate in PA. A possible reason for more frequent logistic support in active parents is parents’ perception towards PA (Rhodes et al., 2020). A systematic review study found that if parents have a positive perception of PA and acknowledge the importance of PA, they are more likely to support their child’s PA (Rhodes et al., 2020). A study also found that parents’ PA is associated with enjoyment and importance of PA in parents of children with DDs (Ku et al., 2020). Thus, in the current study, active parents of children with DDs may have more positive perception towards PA, compared to inactive parents. With the lack of ample evidence in this area, future studies should be done to identify a mechanism that explains why active parents of children with DDs provide more logistic support compared to inactive parents.
Another important finding of the current study was that 26.64% of parents of children with disabilities (n = 319) did not meet the current PA guidelines. This inactive behavior in parents of children with disabilities was also reported by previous studies (Ghim & Ku, 2022; Haegele et al., 2017; Ku & Sung, 2021). A parent’s PA behavior is not only important for their child’s PA but also crucial for their own health (Diaz, 2020; Ghim & Ku, 2022). A nationally representative study conducted by Ghim and Ku (2022) found that active parents of children with disabilities have lower odds of experiencing chronic conditions such as depression, back pain, and obesity. Caregivers of children with disabilities experience unique challenges not shared with caregivers of children without disabilities, such as extra care needs, time pressure, financial problems, and child behavior problems (Park & Nam, 2019; Pinquart, 2018). These challenges may adversely influence psychological and physical health in caregivers of children with disabilities (Gallagher & Whiteley, 2013; Hayes & Watson, 2013; Miodrag et al., 2015). However, PA participation may work as a factor to reduce or prevent negative health conditions in parents of children with disabilities (Ghim & Ku, 2022). Given the physically inactive behaviors of parents of children with DDs, promotion strategies should be created and developed in subsequent studies.
The last finding of the current study was that PPAS-Q provides a three-factor solution, which indicates that it measures three types of parental PA support. Even though previous studies have indicated that parental PA support is a multi-dimensional construct (Rhodes et al., 2020), construct validity evidence for the suggestion was limited, which led to ambiguous understanding of support. However, the current study adds evidence indicating that parental PA support can be measured as a multi-dimensional construct with an appropriate questionnaire. In a systematic review conducted by Trost and colleagues (2013), construct validity evidence of parental PA support was different depending on the questionnaires used. Recently, PPAS-Q was developed to measure parental PA support in children with disabilities, and it has good construct validity evidence (Ku et al., 2022). With this tool, it is possible to measure different constructs of parental PA support, which may lead to deeper understanding of the support. Future studies need to examine the association between different types of parental PA support and PA behaviors in children with disabilities.
Conclusion
The current study confirmed differences in parental PA support between active and inactive parents of children with DDs. In particular, inactive parents of children with DDs less frequently encouraged their child to be physically active and participated less in PA with their child. In addition, they provided less logistic support to their child. These results may suggest that additional strategies should be applied to promoting parental PA support in inactive parents of children with DDs. As child’s age was a significant covariate in predicting co-PA, this also should be considered when developing the strategies. In the current study, 26.64% of parents of children with DDs did not meet the PA guidelines. Parents’ PA behaviors are not only important for parental PA support but also crucial for their own health. Thus, a holistic approach should be considered to improve PA behaviors in the parent-child dyad. With the PPSQ for PCD providing a three-factor solution, the questionnaire can be used to measure different types of parental PA support in parents of children with DDs.
Limitation
One limitation of the current study was that child-related factors such as child’s preference for PA or child’s disability type were not used as covariates in the multiple regression models. A previous study found that parents support their child’s PA because their child likes to do PA (Wright et al., 2020). In addition, there is a difference in parental PA support between parents of children with and without disabilities (Ku & Jin, 2022). Another limitation was that most of the participants were White and Caucasian. However, parent’s ethnicity may be an influencing factor for parental PA support (Columna et al., 2020). When interpreting the current results, these factors should be considered.
Acknowledgments
The author of the manuscript would like to express their gratitude to the parents of children with disabilities who took part in this study.